
Global Health Governance – Representation in a climate of intolerance
Author:
George Njenga Kiai and Madhuri Kamat
Article Type:Article Number: 5
This article, using insights from various sources, aims to provide a glimpse into some of the issues vis-à-vis health governance in some of the multilateral global health initiatives. These include representation, and the climate of increasing intolerance for sexual and reproductive rights that pose the risk of delayed and sometimes cutting off funding to interventions that seek “to leave no one behind” in ensuring access to prevention, treatment and care of diseases.
Introduction
This article addresses the twin challenges of inequitable representation, and social and political polarization faced by some multilateral global health entities. Additionally, it delves into some of the research around these subjects and proposes strategies for enhancing inclusivity in the multilateral global health governance system.
The Need for Broader Geographic Representation
Multilateral global health initiatives are foundational to combating diseases and improving health outcomes worldwide. However, the representation within some of these initiatives at their Board level and their Secretariat often does not reflect the geographic diversity of the populations they aim to serve. Aidspan article’s points out that “Africa, despite bearing over 70% of the world’s HIV/AIDS burden, commands a fractional voice in the Global Fund’s strategic decisions…” Additionally, as per the Yaoundé declaration in 2024 by the the Ministers of Health of High Burden High Impact (HBHI) countries in Africa, “the African region is home to 11 countries that carry approximately 70% of the global burden of malaria”. As per the Global Fund, Nigeria has the biggest malaria burden in the globe, the second-highest number of people living with HIV and the highest number of TB cases in the continent.
Besides two countries in Africa, six countries in Asia account for the highest TB burden in the world as per WHO data in 2022. In Asia, India has the highest TB burden in the world and is also the 12th country with the highest malaria burden. The Asia-Pacific region receives the largest share of Global Fund aid for HIV elimination. Yet, Asia and Africa face underrepresentation within the Global Fund Board dedicated towards the eradication of these three diseases.
It is to be noted that when for the first time in its history, member states had an equal vote in a secret ballot, the WHO got its first Director-General from Africa, Dr. Tedros Adhanom Ghebreyesus in 2017 who was re-elected in 2022. This was possible because the WHO is one of the most decentralized agencies in the United Nations, governed by 194 member states grouped into six regions with their own offices. It enables countries to present their concerns. For instance, during the WHO Executive Board’s meeting in January 2024, countries in the Western Pacific (Malaysia) Eastern Mediterranean (Brunei, Yemen), the Americas (Brazil and Barbados), to name a few, who face their own unique health challenges such as non-communicable diseases (NCDs) called for more to be done on this score. Brunei Darussalam pointed out the need for more precise implementation of tackling NCD and stated that, while “there are established mechanisms for pandemic and health emergencies, such mechanisms for tackling NCDs are more disparate and limited.”[1]
The challenge also lies in the operationalization and mechanics of representation. Each of the six regions has their own regional offices with a regional director appointed by WHO’s Director-General. Each regional committee comprises representatives from the region’s member states’ Ministries of Health (MoHs). The WHO provides expertise where needed. A MOPAN assessment of the WHO in 2017-2018[2], while noting that, “a country office retains some flexibility to respond to the unique context of its operating environment” it is the headquarters that routes the resources to it and this needs to be replaced with a more bottom-up approach.
Resource allocation and funding has always been a fraught issue, given the largely top-down approach in global health initiatives. When countries or internal pressure groups have policies or cultural norms that may conflict with global health objectives, especially in terms of human rights and access to healthcare, global health initiatives find themselves facing increased heat during funding renewals.
Climate of Intolerance for Human Rights
In her presentation at GFAN Africa’s February 2024 meeting on the 8th Replenishment Planning, Claudia Ahumada, Global Fund Manager, Civil Society and Communities Advocacy shared the assessment of the risk landscape (Figure 1).
Figure 1: Global Leaders’ Perceptions of Global Risks in 2024
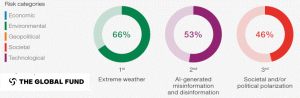
Misinformation and disinformation scored high but these were attributed in the main to be driven by Social Media, Artifical Intelligence technology, etc., but in most of Africa, social media rules the roost with lower AI penetration. Another risk, which was also deemed an urgent threat was social and political polarization. Additionally, Ahumada shared the National Civic Space Ratings of the CIVICUS Monitor 2023, which reported the most targeted among civil society organizations were those that worked on issues of women’s rights and LGBTQI rights. All of these were very much in evidence as elaborated on in the following section.
Conflicts over Sexual and Reproductive Rights
At the 154th session of the WHO Executive Board in January 2023, among the contentious issues was the impartial application of the principles of official engagement of the WHO with non-state actors, with specific reference to the approval for The Center for Reproductive Rights, which was questioned and opposed by many member states. Cameroon, speaking on behalf of 47 member states in Africa, felt the “culture and values” of member states were not being respected. Russia stated that “promoting sexual rights” is not part of the WHO mandate. On the other hand, supporters of the WHO move, like Mexico on behalf of 25 member states (centred majorly in Europe and Latin America), accused the member states who were raising objections of “politicizing routine decisions”.[1] The decision on engaging with the organization stands postponed for now. Another controversy erupted over the use of the term “WHO LGBTQI+ community” in a human resources report tabled at the board meeting.
Support for abortion and “promotion of LGBTQI issues” by PEPFAR – which in collaboration with the Global Fund represents about two-thirds of donor support worldwide for HIV prevention, care, and treatment – were also cited as reasons for opposing its funding renewal. Although it got passed after bipartisan support in the US Congress and the US Senate, the renewal period continued to be pared down to a year as opposed to the five-year term it enjoyed in earlier years.
However, there was something far more insidious at work in the above challenges to WHO and PEPFAR: misinformation and disinformation. And they did not stem from social media or AI but vested interest groups. In the case of the WHO controversy, the specious claim made was that the recent agreement regarding pandemic preparedness would be “used to undermine national laws related to abortion.”[2] There was a « sustained campaign » by the same organization behind the specious claim, which made another one against PEPFAR supporting abortion in countries in Africa when in fact abortion is illegal in Africa.[3]
The misinformation also disregarded the commitments to sexual and reproductive health and reproductive rights enshrined in the Programme of Action of the International Conference on Population and Development, the Beijing Declaration and Platform for Action. These were also reiterated by the UN General Assembly’s Political Declaration on HIV and AIDS, 2021. It noted with concern that sub-Saharan Africa, is the region where « five out of six new [HIV] infections among adolescents aged 15–19 years are among girls, that adolescent girls and young women (15–24 years) account for 24 per cent of HIV infections despite representing 10 per cent of the population, and that AIDS is the leading cause of death for adolescent girls and women aged between 15 and 49 years. » In short, the burden of the AIDS epidemic’s devastating effects falls particularly on women, adolescent girls and children.
Global Health Alliances
In the face of such mounting challenges and with communities and countries in the Global South seeking a greater say in decision-making, the formation of alliances such as One Health, the Global Alliance against AIDS, the Lusaka Agenda and the Global Public Investment (GPI) funding framework underscores the importance of collaborative efforts in tackling global health issues. These alliances bring together countries, international organizations, civil society, and the private sector to address health challenges through a unified approach. Countries play a crucial role in these alliances by contributing resources, sharing expertise, and fostering political will to prevent, detect, and respond to health threats. By actively participating in and supporting these alliances, countries can help ensure a coordinated response to health crises, leveraging collective strengths to achieve greater impact. Let us examine some of the research on issues faced by multilateral global health governance.
How countries can become bridges
In January 2024, the Center for Global Development brought out a policy paper entitled Mind the Gap Bridging the Divide between Cooperation Providers, which suggests that countries can become the needle to sew together disparate entities across the developmental divide. It offered a model of bridging functions (Figure 2):
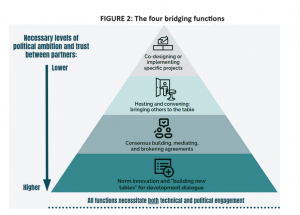
The paper went on to state that technical collaborations can continue even when political trust is low. There can be joint implementation on select thematic areas.
One can see how this is already working out in, for instance, the One Health Alliance, which emphasizes the interconnectedness of human, animal, and environmental health, promoting cross-sectoral collaboration to achieve optimal health outcomes. Another is the Lusaka Agenda 2023 where a timeline and path has been set towards “a joint long-term vision of domestically-financed health systems and Universal Health Care that leaves no one behind”. It involves GHIs “jointly engaging with pathfinder countries with different levels of systems maturity. Ghana, Canada are the countries that have stepped up to be the “bridges” by forming an informal steering group with Amref Health Africa to initiate the implementation of the Lusaka Agenda and engage stakeholders such as GHIs, civil society organizations, and a broader spectrum of donors and implementing countries.
Enhancing representation and engagement
The Chatham House provides insights into building more inclusive global governance, stressing the outdated nature of current multilateral systems and the importance of inclusivity for transformational change. The changing dynamics of global governance, characterized by the rise of non-state actors and the diffusion of power among a wider array of states and actors, underscore the complexity of achieving meaningful representation. The challenges of coordinating responses to global issues, such as health crises, through traditional governance structures are becoming increasingly evident.
However, a distinction as forwarded in the book, Rethinking Participation in Global Governance – Challenges and Reforms in Financial and Health Institutions, published by Oxford, 2022 needs to be made between, “voice [opportunities] and influence.” The latter is having a decision making (rule-making) role in policies, processes and outcomes. As the book points out, what prevails today is “democratic legitimacy” but it has to translate into “enhanced responsiveness-based legitimacy.” Engagement with governance bodies is likely to fall off when participants realize they may have a voice, but no influence but if the former is expanded with an assurance of the latter, it can lead to a rise in the political costs of expanding opportunities.
Human Rights in health governance
Protection of vulnerable groups is expected of the state, and non-discrimination is enshrined in international covenants, which states must actualize. Accessibility, besides non-discrimination encompasses physical, informational and economic dimensions. To understand more on this subject, Health and Human Rights Journal offers an in-depth analysis of health governance in the face of ethical challenges.
The Way Forward
Multilateral global health governance requires a multifaceted approach, focusing on geographic, operational, and ethical dimensions.
- Improving Diversity in Representation: Advocate for and implement changes in the governance such as their Board, Committees and Secretariats structures of global health initiatives to ensure more equitable representation from Africa, Asia, and Latin America. This includes revising voting mechanisms, allocation of seats, and engagement strategies to reflect the diverse needs and contributions of these regions.
- Navigating Cultural and Ethical Challenges: Develop advanced strategies for engaging with countries leadership and communities with contentious policies, focusing on diplomatic engagement and advocacy that prioritize health outcomes while respecting cultural differences. This requires a balanced approach that supports on-the-ground health initiatives without compromising on ethical standards.
With global governance still largely inter- and trans-governmental, it is finally political priorities amidst growing nationalist protectionism and the rise of conservative lobbies, which will determine whether a more equitable, responsive, and ethically conscious global health governance becomes an effective reality. From the macro- to micro-levels, the pushback will have to also come from the community level. As community-led health interventions including community-led monitoring become the flavour of the season, it’s important for cross-learning between civil society and community-based organisations to ensure their voices not only get heard at fora that matter but lead to action at the ground. In the words of community leaders quoted in the UNAIDS World AIDS Day Report 2023, “We should not be seen as a target of interventions, but as the principal intervention. We should not be seen as the problem, but as the key to the solution.” With elections scheduled across the globe, it is their vote that will determine the future direction of global health governance.
_____________________________________________________________________
[1] Non Communicable Disease Alliance’s Analysis of the 154th session of the WHO Executive Board.
[2] https://www.iodparc.com/wp-content/uploads/2023/05/WHO-Report.pdf
[3] Cullinan, Kerry, Row Over Reproductive Rights Group at WHO Executive Board ‘Undermines’ Secretariat and ‘Science-Based Approach, Health Policy Watch – Independent Global Health Reporting, January 29, 2024.
[4] Ibid.
[5] Cullinan, Kerry, Lives Are At Risk as Anti-Abortion Groups Attack HIV Programme PEPFAR, Health Policy Watch – Independent Global Health Reporting, June 20, 2023.
