
Global Fund Technical Review Panel observations on funding requests from Windows 1, 2 and 3
Author:
Aidspan
Article Type:Article Number: 3
On 18 October 2023 the leadership of the Global Fund Technical Review Panel made a presentation to the World Health Organization Joint Working Group on the lessons learned from and observations on Funding Requests for Windows 1, 2 and 3 of Grant Cycle 7. This article summarizes that presentation together with key comments made during the Joint Working Group’s discussion.
Introduction
The Technical Review Panel (TRP) is the independent body which assesses countries’ funding applications to the Global Fund and recommends their approval or “reiteration” or revision and resubmission. On 18 October 2023, the TRP presented its findings and observations on the three application Windows to the World Health Organization (WHO) Working Group which comprises the Global Fund, UNAIDS and its co-sponsors and other technical and financial partners such as Expertise France and others.
The TRP’s scope of work during Grant Cycle 7 (GC7) application Windows 1,2 and 3 was as follows:
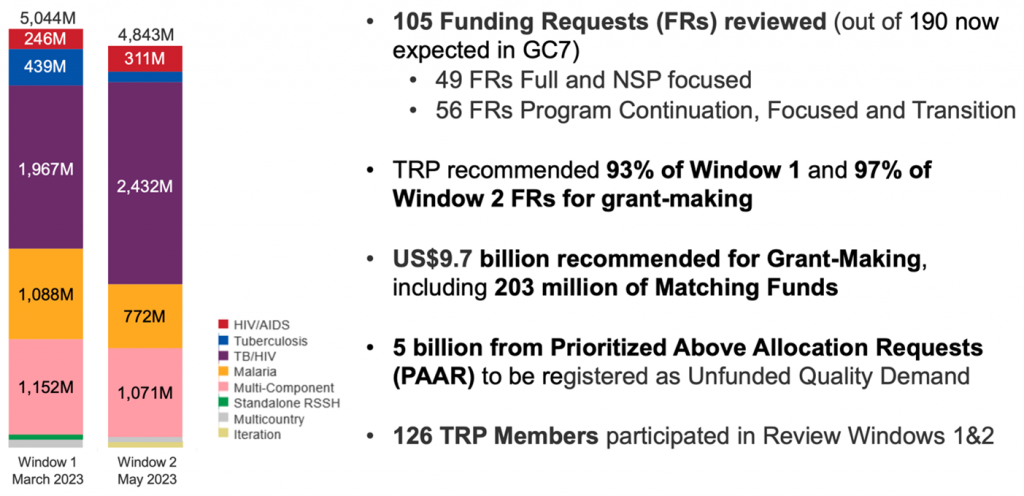
Windows 1 and 2 overview
Ending AIDS, TB and Malaria
The TRP presented the following overall contribution of Windows 1 and 2 FRs to the goal of ending AIDS, TB and malaria:
Ending AIDS:
- Increased attention to prevention and focus on adolescent girls and young women and other key and priority populations.
- Strong test and treat programs including innovations towards meeting the 95-95-95 targets – often leveraging opportunities created by the COVID-19 pandemic.
- Suboptimal use of available data and evidence to justify investments.
- Applicants struggled with prioritization and differentiation within the context of a limited GC7 allocation and domestic fiscal space.
Ending TB:
- Continued efforts to find more people with TB by deploying new technologies for diagnosis and differentiated approach to reach key and vulnerable populations including matching funds, but further evidence-based optimization is needed.
- Gaps in/between the TB diagnosis, treatment, and prevention cascades should be addressed to ensure a continuum of quality TB care.
Ending Malaria:
- Progress towards elimination in low-transmission settings.
- Stagnation or deterioration in progress in reducing malaria burden in high burden settings.
- Positive move towards increased stratification and interventions – further progress still needed.
- Additional resource mobilization needed. The lack of resources for adequate coverage of essential interventions in many countries presents a significant risk to overall progress.
Global Fund Strategy
The TRP presented the following overall contribution of Windows 1 and 2 FRs to the Global Fund’s Strategy:
People-centred integrated systems health:
- Increased investments in resilient and sustainable systems for health (RSSH) and complementarity with the COVID-19 Response Mechanism (C19RM) but still with an emphasis on systems support rather than strengthening.
- Encouraging shift towards expanding and integrating community health workers and other community-based health workers.
- Country Coordinating Mechanisms and Ministries of Health should take a greater role in coordination of the full range of partners and ensure stewardship of national programs.
- Applicants should maintain an up-to-date mapping of health partners and donors and supported activities and provide a complete picture of RSSH investments and activities of in-country partners.
Engagement and leadership of most affected communities:
- Positive shift in integrating community systems and responses, stronger role and voice of people and communities living with and affected by the diseases. But more is required on community-led monitoring and social contracting for sustainability.
- Structural barriers remain, including continuing challenges in enabling the legal structure for social contracting.
- Increasing criminalization of key populations (KPs) led to challenges in prioritizing interventions for KPs though innovations were used in the language to continue service delivery for them.
Health equity, gender equality and human rights:
- Acknowledgement of barriers to care and equity, human rights and gender (EHRG) assessments do not always translate into investment in concrete programmatic activities – vastly under-prioritized and underfunded.
- KPs often discussed as ‘one’ homogenous population without consideration of differentiation and intersectionality between and within KPs.
- Insufficient considerations for inequities based on various dimensions to respond to underlying social and structural drivers of these inequities.
- More effort is still needed in utilizing findings from gender, human rights and legal assessments to inform the FRs and related prioritization of interventions.
Mobilizing increased resources:
- There is a notable improvement in domestic resource mobilization and co-financing in some portfolios but proposed activities do not always reflect good value for money or sustainability.
- There is continued dependence on external funding and limited progress on tracking HTM spending at sub-national levels.
- Blended finance projects, often with a focus on Universal Health Coverage expansion, can allow progress towards more integrated strategic purchasing of health services – The virtual pooling of Global Fund investments with World Bank loans in several Challenging Operating Environment (COE) countries was welcome.
- Slow progress on social health insurances (SHI) limits integration of ATM into benefit packages; there’s a need to ensure social contracting for key services outside SHIs’ purview.
Cross-cutting observations
The TRP’s cross-cutting observations from the Windows 1 and 2 FRs were:
- There was a notable improvement in the overall quality of FRs. However, while there was progressive use of national data to guide the selection of interventions, significant prioritization and ambition challenges remain as allocation budgets are spread too thinly or essential interventions are front-loaded.
- High program management costs remain a concern, while: (i) prioritized above allocation requests (PAAR) include critical interventions; (ii) there are examples of PAAR amounts exceeding double the size of the actual country allocation; and (iii) EHRG investments are commonly relegated to PAAR.
- There are some examples of increased optimization and precision in ATM responses but more progress is needed.
- There is a general increase in the quality and quantity of RSSH investments; however, concerns remain about the slow shift of investments to system strengthening.
- Increased focus on integration with commendable examples in some areas but missed opportunities in others (e.g. reproductive, maternal, newborn, child and adolescent health (RMNCAH), sexual and reproductive health (SHR), primary/public health care and human resources for health).
- Better collaboration is required among partners at country level, especially during grant implementation.
- There is a need for further efforts in market-shaping and the introduction of health products.
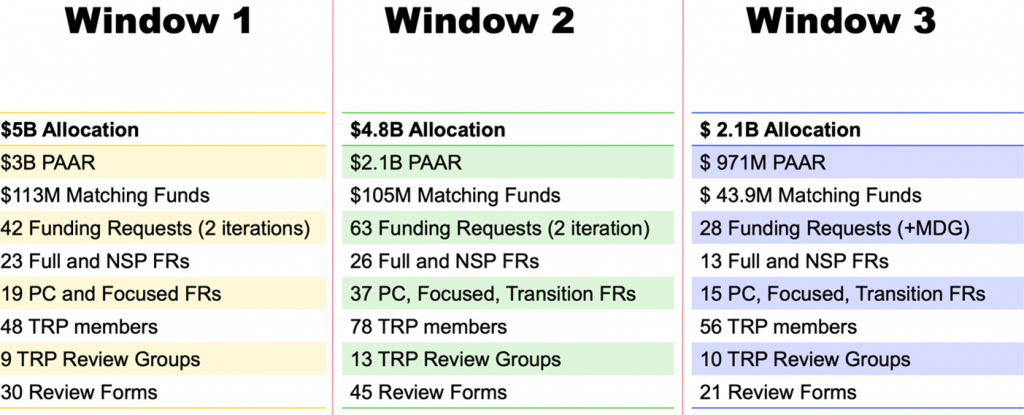
TRP Window 3 Overview
TRP reviewed 28 FRs:
- $2.1 billion within the allocation amount;
- $43.9 million in matching funds; and
- $971 million under PAAR.
TRP Review approaches:
- 13 Full Review and Tailored for National Strategic Plans (NSP) FRs; and
- 15 Program Continuation, Focused and Transition FRs.
Window 3 outcome:
- All FRs were recommended for grant-making, representing 15.9% of the total GC7 allocation; and
- In 2023 TRP reviewed nearly 90% of the total communicated GC7 allocation amount.
WHO Working Group comments
The following key comments were raised during the Working Group discussion:
- The rise in the amount of Unfunded Quality Demand (UQD) under PAAR can be explained by the pressure on the need for prioritization within limited allocation amounts and restricted fiscal space. In Windows 1 and 2, particularly for malaria, applicants could not afford the full demand of commodities within allocation. This is an example of the costs of commodities and implementation driving what would be put into the PAAR. There is a tendency for some important interventions, particularly for KPs, being relegated to PAAR, for example EHRG interventions. The major driver is the reality of the funding context.
- Gaps in the TB diagnosis, treatment, and prevention cascades should be addressed to ensure a continuum of quality TB care. In the FRs TB interventions need to be better linked to the targets. The TRP leadership would like to encourage applicants to focus on more continual TB care.
- Africans are struggling to procure new technology due to limited budgets, human resources and the weak capacity of national health systems. Optimization could be a way forward, e.g., countries conducting laboratory network optimization assessments and using country-based evidence to decide on the distribution of new technology with limited human resources in the appropriate place and setting.
- Private sector engagement is one of the challenges for TB, especially civil service organisations (CSOs). The Global Fund tries to encourage Africans to capacitate the CSOs as the private sector and embrace them to improve the TB program data. This applies to HIV as well. More private sector engagement in HIV care and treatment programs would be beneficial.
- On people-centred integrated systems for health, there is still too much emphasis on system support rather than strengthening. Due to the overall slowdown during COVID-19, countries had to put in more support even for C19RM, as well as for GC7. The TRP leadership encouraged Global Fund partners to work across the partnership for more impactful RSSH implementation work, driving more system strengthening.
- On inclusion of co-morbidities (mental health and non-communicable diseases [NCDs]) in FRs, some interventions were proposed together with TB treatment, but not many. TRP leadership would like to see more of the inclusion of co-morbidities to improve the quality of care in TB. A lot of language on integration of co-morbidities was also noticed in HIV FRs, mostly for screening, but not enough ambition for management of co-morbidities to be able to procure what is needed. Increasing mention of integration with mental health was noted as well, though this is still in the initial and innovative phase. For malaria, there was a lot of integration at community level, with malaria packaged with pneumonia and other childhood diseases. In terms of application of longevity approaches in HIV linked to NCDs, there is room for improvement.
