
Global Fund Grants to the Republic of Zambia
Author:
Oliver Campbell White
Article Type:Article Number: 5
Business as usual cannot continue
The Office of the Inspector General’s audit report on the Global Fund grants to Zambia makes for essential reading because, against the background of poor performance of programs managed by the major Principal Recipient, the Ministry of Health, it leads the reader to conclude that the Global Fund must rethink some policies and practices. First, there appears to be a need for more rigour in routine performance assessment. Second, given the absence of any mention of the Country Coordinating Mechanism (CCM) in the report, the role and performance of the CCM must be reconsidered; and this may impact the work and views of the Technical Review Panel when the forthcoming funding requests are submitted. Third, the country allocation policy may also have to be reconsidered because the Global Fund has a duty to invest its resources wisely; and, given the performance of the larger grants in Zambia, there cannot be justification to increase disbursements until corrective action has been observed.
Background
On 24 November 2022 the Office of the Inspector General (OIG) published its report on the audit of Global Fund grants in Zambia which covered Principal Recipients (PRs) and Sub-Recipients of the Global Fund supported programs for the NFM2 and NFM3 grants from January 2019 to December 2021.
The amounts of Global Fund grants disbursed in the full period under review are not stated in the report. Signed and disbursed totals for the malaria and HIV/TB programs (but not by PR) for the periods January 2018 – December 2020 and January 2021 – December 2023 are shown in a table but the January 2021 – December 2023 amounts do not tally with that shown in the Global Fund data explorer.
The report provides the following table on the disease burdens:
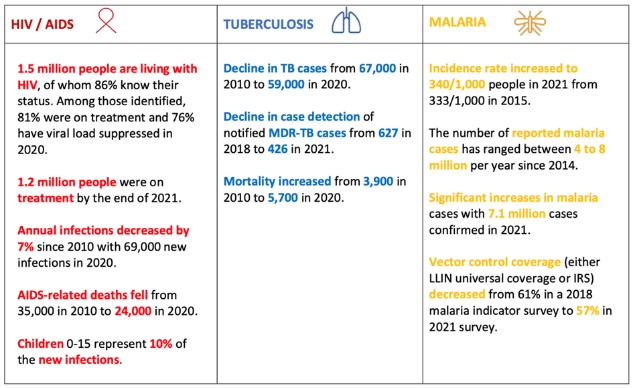
While the table provides information over the periods stated, it does not provide the reader with data on progress during the period since the previous audit review published in December 2017.
First Finding
The first finding is stark and unambiguous: “Declining performance in malaria highlights the inability of Global Fund grants to support the achievement of intended objectives. The malaria grant set ambitious elimination targets that have not been achieved. Rising rates of morbidity and mortality are linked to issues with vector control implementation, sub-optimal community case management, declining knowledge of malaria in the general population and the government’s lack of prioritization of the malaria response.”
Some successes and good practices are noted. However, the 2017 national malaria plan sought to eliminate the disease by 2019 before pushing the target back to 2021. These targets were not met as malaria incidences actually increased from 2018 levels, showing the country has moved further away from achieving elimination over the past five years.
The report links the drastic decline in malaria programmatic results to four root causes:
- Challenges in vector control implementation that cause operational gaps, reducing the effectiveness of activities to reduce malaria cases. The audit noted: (i) that the government’s local procurement processes and supply chain issues delayed the roll-out of activities, reducing effectiveness; and (ii) a lack of analysis to determine the effectiveness of the LLIN mass campaign.
- The missed opportunity to leverage community case management to tackle increases in cases and deaths.
- A growing gap in malaria knowledge that impacts the effectiveness of program interventions.
- Reduced government prioritization and ownership over malaria interventions that result in a failure to deal with key gaps in activities.
The audit report’s commentary on cause 4 is of the utmost importance for understanding the situation and the difficulty of remedial action. It begins by stating that: ”An effective national program for malaria requires the government to prioritize and demonstrate ownership over the program. But in Zambia, the OIG noted the opposite is occurring with declining prioritization and ownership over the malaria response. This contributes to gaps in funding, planned domestic procurements going unrealized and delays in resolving key programmatic recommendations.”
Second Finding
The second finding is that “The HIV program has made significant progress in tackling HIV treatment for adults but issues with assessing ART attrition, as well as significant delays, poor performance and limited scale-up of adolescent and young people (AYP) and key population (KP) activities threaten to stall and reverse programmatic gains made.”
It goes on to note that challenges in three key areas of the HIV response threaten to reverse programmatic progress made:
- The picture of ART attrition is unclear and this undermines the ability to effectively assess and tackle non-adherence.
- Delays, poor performance and limited scale-up of adolescent and young people (AYP) activities, notably implementation challenges and delays of over 19 months of key AYP activities under the Ministry of Health (MOH) for NFM 3.
- Slow progress in tackling key issues and scaling-up the KP program since the 2017 OIG audit.
With regard to item 3, the report notes that: “There are still high levels of stigma, denial and discrimination that impact the development of comprehensive national policy and strategy. In addition, there is a significant lack of government ownership over the key population program with limited domestic financing for activities.” This makes for disappointing reading after so many years.
Third Finding
The third finding is that: “There has been continued progress in reducing cases of drug susceptible TB with strong results for interventions on TB-HIV comorbidity. Multi-drug resistant (MDR) TB, however, is a growing problem in Zambia with increased estimated cases coupled with declining notifications.” The report explains that the low MDR-TB detection rates are due to issues with the use of diagnostics and challenges in active case finding.
Fourth Finding
The fourth finding is particularly worrisome: “Ineffective design and implementation of the Ministry of Health (MOH) Program Management Unit (PMU) structure results in gaps in financial management, internal audit, and HR management.”
The OIG noted that the second PR, the Churches Health Association of Zambia (CHAZ) “had well designed Sub-Recipient (SR) management policies, guidelines and procedures. In the OIG’s sample-based review, robust monitoring and oversight was evidenced that resulted in timely supervision and feedback to SRs and quick retirement of advances. The OIG also observed adequate financial controls in place at CHAZ, with no unsupported expenses or material irregularities found in the sample of transactions reviewed.”
In contrast, despite significant investments, the MOH PMU had the following persistent and material issues in its functioning:
- Sub-optimal management and oversight of SRs resulting in significant outstanding advance balances.
- Issues with financial recording and clearance of PMU staff balances resulting in a large unresolved imprest balance.
- Gaps in key controls and processes around fixed asset management leading to significant variances in records.
- Weaknesses in financial management systems, accounting, and reporting leading to unsupported financial expenditures, incorrect accounting, and gaps in financial oversight.
- A lack of monitoring of internal audit findings and issues with human resource (HR) payroll processes.
- Gaps in governance, oversight and performance management resulting in weak management of grants in key areas.
Fifth Finding
The fifth finding is that: “The OIG audit in 2017 had highlighted critical issues in procurement and supply chain management (PSM). While there has been some progress since then, significant issues have persisted due to limited implementation oversight and lack of senior MOH ownership over PSM issues contributing to stock-out risks for malaria and HIV commodities.”
With respect to PSM, the OIG noted repeat issues in four key areas from prior reviews:
- Persistent data quality, analysis and system issues impacting assumptions used in forecast planning. In addition, there are unexplained discrepancies between the forecasted demand and the eventual annual supply plans for ACT, RDT and core ART that are used to guide procurements, rendering the output of quantification and forecasting obsolete.
- The two regional hub sites that were visited remain under-utilized for the three diseases. Malaria commodities are still not part of the hub stock keeping strategy, meaning that all routine health facility orders for malaria products by-pass the regional hubs for processing at the Zambia Medicines and Medical Supplies Agency (ZAMMSA) HQ. A significant quantity of commodities still flows directly from the ZAMMSA central warehouse to the district and provincial health offices. Operational issues were noted with the regional hub warehouse management system that is not connected to ZAMMSA. In addition, the regional hub stock count variances are not investigated and stock-outs were noted at the regional hub and health facility levels.
- The Electronic Logistics Management Information system (eLMIS) is still not rolled out fully with health facility coverage at just 45%. In addition, the eLMIS is not interoperable with other key PSM data systems like the national warehouse management system, leading to gaps in oversight.
- The OIG noted variances in monthly stock reconciliations at ZAMMSA that were not investigated by warehouse staff. This increases the risk of stock mismanagement and loss.
OIG is of the view that the key PSM issues persist due to limited implementation oversight and a lack of MOH senior management ownership over strategic plans. In support of this, the report notes:
- The lack of clear roles and responsibilities and capacity in the MOH over key elements of PSM operations.
- Gaps and delays in development and implementation of national strategic and operational plans and policies.
- Weak governance structures that prevent the ability to effectively monitor, address and escalate PSM issues.
The finding concludes by stating that the PSM challenges are contributing to prolonged malaria commodity stock-outs as well as stock-outs and continual stock-out risks for HIV commodities.
Agreed Management Actions
The agreed management actions (AMAs) for each finding are as follows:
- The Global Fund Secretariat (Secretariat) will support the MOH to assess factors which are hindering Malaria programmatic performance, developing tailored interventions as necessary, specifically for vector control to address challenges in the mosaic approach to reduce gaps to coverage and improve the outcomes of future campaigns. The due date is 30 June 2023.
- The Secretariat will support the MOH to conduct: (i) a nationally representative Integrated Biological-Behavioural Surveillance Survey (IBBS); and (ii) a nationally representative KP size estimate and mapping using multiple methods (for sampling and extrapolation) in line with the WHO/UNAIDS guidelines with the goal of improving data on key populations to support programmatic design. The due date is 31 December 2023.
- The Secretariat will work with the MOH to strengthen the training and supervision of Community Health Workers involved in Active Case Finding for TB. The due date is 31 December 2023.
- The Secretariat will work with the MOH in a full redesign of the MOH PMU structure and its relationship with the MOH to strengthen operational management by the PMU and oversight by the MOH in time for the next grant cycle beginning 1 January 2024. Specifically:
-
- By 30 September 2023, through leveraging the outcomes of the OIG audit along with conducting and leveraging an independent assessment of the PMU MOH operating model, the MOH will redefine the PMU structure and implement revised reporting lines and reporting processes, and key performance indicators across PMU staff and enhanced PMU oversight; and
- By 31 Mach 2025, an annual performance review on the PMU after the redesign is implemented.
- The Secretariat will support the MOH in strengthening the governance, oversight and roles and responsibilities over health related PSM processes under the MOH grants. Specifically:
-
- by 31 December 2023:
-
-
- Establishing a national PSM governance oversight mechanism reporting to the Permanent Secretary for monitoring the implementation of the national supply chain strategy; and
- Defining roles and responsibilities of national stakeholders over the full national health PSM cycle including cross cutting governance and oversight, quantification and forecasting, supply planning, procurement (international and domestic), supply chain and LMIS systems.
-
-
- by 31 December 2024, the operationalization of the PSM governance oversight mechanism providing oversight over the national supply chain strategy.
Commentary
This audit report is unambiguous; and two stark factors stand out. First, the MOH has failed to function adequately as a PR; and, second, the Secretariat appears to have been lenient and not exerted sufficient pressure on the MOH and the CCM.
To put those factors into context, here are the AMAs from the December 2017 audit report on Zambia:
- Quality of Services: The Secretariat will work with the MOH and key stakeholders to monitor implementation of the new grants. Specific focus will be given to activities to improve:
- diagnostic capacity;
- HIV and TB testing and referral;
- ART patient monitoring;
- MDR TB outcomes; and
- malaria vector control outcomes.
- Data Quality: The Secretariat will work with the MOH and key stakeholders to address the underlying system weaknesses prioritized in the new grants and noted in the report. Specific attention will be given to improving stock management and last mile distribution.
- Supply Chain: The Secretariat will work with the MOH and key stakeholders to address the underlying system weaknesses prioritized in the new grants and noted in the report. Specific attention will be given to improving stock management and last mile distribution.
- Governance: The Secretariat will work with the MOH, the CCM, and key partners to develop a plan to strengthen oversight, including of the PMU.
Readers will notice that the AMAs in the 2022 audit report are about working with the MOH to do very much the same thing as the AMAs in the previous audit report. That suggests to us that, despite whatever advice and pressure from the Secretariat and technical assistance over five years, the MOH has not improved in its functioning as a PR in over ten years.
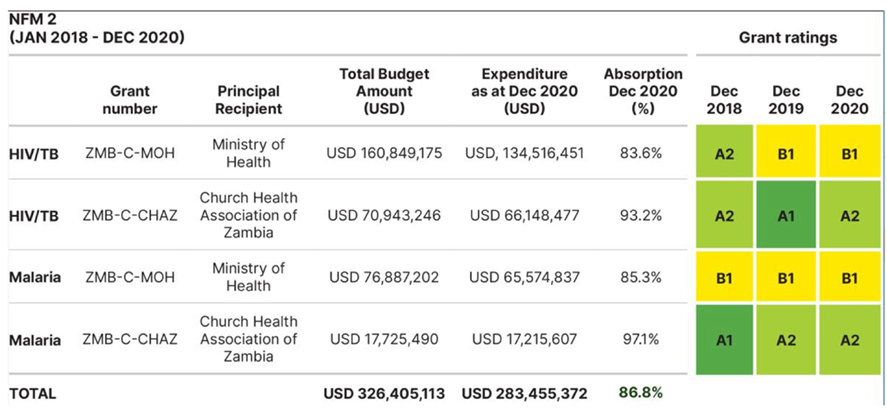
The Secretariat appears to have been lenient. Not only is grant performance poor, Section 3.1 of the audit report states that: “Historically, Global Fund grants in Zambia have performed well against targets, as shown in the below grant ratings determined by the Global Fund Secretariat. The Secretariat approach to rating grants is complex, considering numerous factors. The ratings for the Ministry of Health highlight a disconnect between the OIG findings in key areas and the overall ratings given per grant.”
There most certainly is a ‘disconnect’ between the OIG findings and the Secretariat’s ratings; and it is a pity that the OIG diplomatically avoided saying more about this.
We are therefore left wondering why the Secretariat reports progress as relatively satisfactory when the OIG clearly rates it as not. And, given the poor state of Zambia’s economy and the likelihood that the MOH will have no increase in funding in the foreseeable future, it is difficult to see how the AMAs will be properly fulfilled.
On the subject of the AMAs, the timings of completing AMAs 4 and 5 (31 March 2025 and 31 December 2024) are such that they will not have the required remedial effect for the immediate forthcoming grant cycle.
A surprising omission in the audit report is any mention of the CCM. The CCM is central to the Global Fund’s approach to grant funding request preparation, evaluation and approval and to subsequent performance monitoring and evaluation. Why, therefore, is Zambia’s CCM not mention anywhere and not included in the AMAs? We can only deduce that the CCM too is not functioning properly. leads us to think that some Global Fund policies and processes require review and adjustments. First, the disparity between the Secretariat and OIG performance ratings suggests a need for more rigour in routine performance assessment.
Second, given the absence of any mention of the CCM in the report, perhaps the role and performance of the CCM must be reconsidered – or the AMAs adjusted to include the CCM. In Zambia’s case, the apparent ineffectiveness of the CCM may impact the work and views of the Technical Review Panel when the forthcoming funding requests are submitted.
Third, the country allocation policy may also have to be reconsidered because the Global Fund has a duty to invest its resources wisely; and, given the performance of the larger grants in Zambia, there cannot be justification to increase disbursements until corrective action has been observed.
We shall monitor Zambia’s progress with interest.
