
Allocation on a Budget – The What and How of it.
Author:
Madhuri Kamat
Article Type:Article Number: 4
The Allocation Methodology was one of the most awaited presentations and there was a host of views on what more needs to be finessed amidst worries about lower replenishment scenario. Everyone will await with bated breath the replenishment round when it happens and hope that the Global Fund will attain the targets and then some.
Introduction
As the Global Fund faces its eighth replenishment round, it is not surprising that its allocation methodology, which was the subject of intense and lengthy conversations at different fora of the Global Fund, including its 51st Board meet and retreat was back to raise heat at the Malawi 52nd Board meet.
Allocation Methodology
To understand how the allocation methodology works and what it’s all about you can read our previous article on it Global Fund Allocation – A Brave New Method in the Offing? or this allocations faqs put out by the Global Fund.
Summary of Changes
A summary of the changes in the allocation methodology as of now is to be found below.
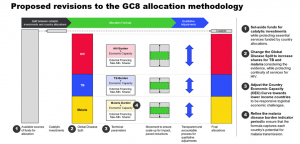
Revised Allocation Methodology
|
Principles Guiding the Allocation Methodology Transparency and flexibility is key for the Global Fund, which is why it has tried to ensure that specific country contexts requiring adjustments can be made possible by ensuring that the allocation process is open. This goes hand-in-hand with adaptability that takes into account changes required in response to new data, global economic shifts, and emerging health challenges. Eventually, the aim is maximizing impact to ensure that the funding priorities get most bang for the buck, of course, but also attain the health outcomes at the scale required and are maximized.
|
|
Global Fund Allocation Methodology Areas Country Economic Capacity Curve Adjustments keeping in line with the principle of adaptability reflects shifts in countries’ economic status, recognizing that global economic challenges disproportionately affect lower-income countries and aims to protect allocations to lower-income countries facing increased economic pressures. Disease Burden Formula Refinements maintains a focus on disease burden as a primary factor. This necessitates the incorporation of recent epidemiological data to capture the current state of each disease as well as to adjust for potential reversals in disease control due to changes in interventions or emerging threats. Qualitative Adjustments Process as the name goes addresses factors not fully captured by quantitative metrics, such as health system resilience, climate change impacts, and cross-border health issues. This is continuing with the flexibility and adaptability principles so as to ensure that allocations consider the unique challenges and contexts of each country. |
The following section details what’s at the heart of the allocation methodology and the kerfuffle about it.
Global Disease Split
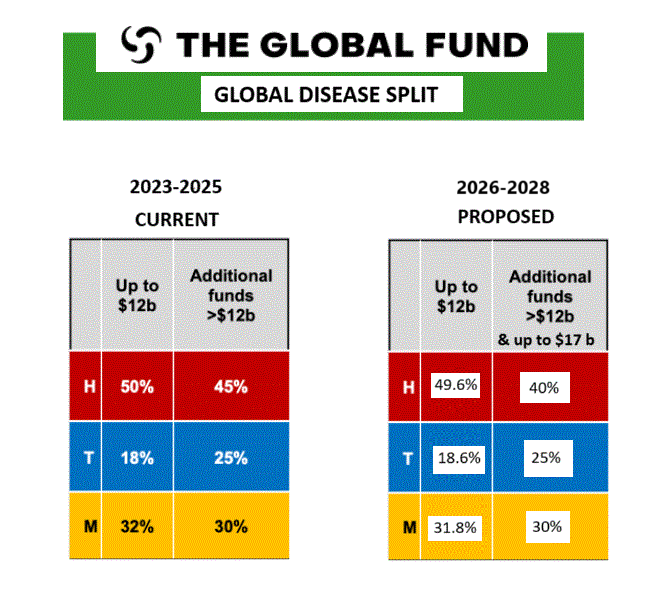
As can be seen from the above, in the allotment up to $12 billion there is only a blink-and-you-miss-it increase for TB and a decrease for malaria and HIV, while remaining steady for the other two diseases vis-à-vis the allocation above $12 billion and more. It was clearly stated in the Independent Evaluation sought by the Board to keep “an upfront split in the Allocation Methodology” and revise the global disease split (GDS) “in favor of TB to better align with the epidemiological context.” However, the response at that time was that the epidemiological context had to be seen along with other factors such as the financing landscape, economic capacity, the cost of essential programming, previous funding levels, and the impact of investments.
Stakeholder Feedback on what the Global Fund is doing and what it needs to do or not
At the 51st Board meet in Geneva; the Global Fund had been asked by stakeholders to appoint a Task Force to review the GDS as part of a transformative approach, which could develop new frameworks for the global disease split, ensuring that these are informed by comprehensive data analysis and reflect true needs.
Global Disease Split
Concerns were raised on the increase in share for the $12 billion – $17 billion replenishment level being gradual and inadequate while being conditional to the eighth replenishment amount in the below $12 billion range. It was also pointed out that there are no recommendations regarding what happens to the GDS in a lower replenishment scenario.
TB
Evidence shows that TB funding has a ripple effect:
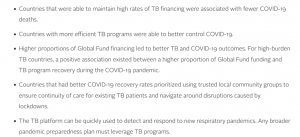
This was confirmed by a study using sources such as the World Health Organization (WHO), Global Fund, Our World in Data, and domestic health ministries, found that “countries with better TB program strength going into the pandemic fared better with COVID-19 than those with poorer TB treatment. It was found that countries that recovered their TB program strength (as measured by TB treatment coverage percentages) to or above pre-pandemic levels fared better in terms of COVID-19 pandemic incidence and death.” The case studies revealed that common factors across resilient TB platforms in dually successful COVID-19 and TB countries, included “community trust, co-epidemic responses that were able to maintain continuity of care, sustained innovation, comprehensive communication across public and private sectors, and maintenance of donor support for TB programs through the pandemic.”
Given that TB is a public health challenge it was felt that the formula being used in allocation to TB in the GDS did not adequately reflect the true costing needed for TB to be tackled effectively given the rising tide of drug-resistant TB and the need to scale up diagnostic tools and access.
HIV
There was support for the Global Fund proposal to review the Key Populations Adjustment in the GC8 Allocation Methodology. However, it was requested that it be comprehensive including at Stage 1 of Qualitative Adjustments: i) thorough assessment of the existing matrix of proposed indicators and their thresholds, ii) the selection of subpopulations that are to be included, and iii) sustainability considerations. The review should also mirror the proposed changes in the allocation methodology and Sustainability Transition and Cofinancing policy, including a) GDS adjustments, b) shifts in the CEC (Country Economic Classification) curve, and c) any alterations in the transition policies.
At Stage 2 of Qualitative Adjustments, there were calls for understanding the country context through use of subnational HIV incidence, prevalence and treatment coverage among key populations. This is especially important given that there’s a worrying trend towards resurgence in that the number of new infections outside sub-Saharan Africa exceeded that in sub-Saharan Africa. There was also a demand for additional formulaic qualitative adjustments to meet the challenge of the critical gaps in eliminating vertical transmission and improving the paediatric HIV treatment cascade. The use of the mother-to-child transmission rate was suggested. This is in light of the vaulting rise in pediatric HIV and vertical transmission and has been a demand from constituencies, which also want for adolescent girls and young women (AGYW) to be part of the adjustment criteria. For instance, in sub-Saharan Africa region, 3,100 AGYW are infected each week.
Malaria
There was emphasis on the need to retain the clause that allows the Secretariat to recommend to the Board, when necessary, that a country continue to receive funding in the event of an “unusual increase” in malaria cases even if such a country has been deemed malaria-free as per criteria or because it is not eligible as per income-level criteria. This is to shore up support and prevent reversal of gains made in eradicating malaria in these countries. There was also a recommendation that in the event that the malaria incidence rate is higher than the set average, and the increase is significant, there may be a need for further adjustments through the qualitative adjustment stage. As an important point was made that factors beyond disease burden also may be in play such as humanitarian crisis and coverage gaps.
About malaria, some constituencies were not in favor of the malaria vaccine as they believe that countries should consider trade-offs since vaccines seem expensive, and instead prefer long-lasting insecticidal nets (LLINs). Opinions on this matter diverge, too, especially regarding the vaccine’s effectiveness after four doses. Some argue that the vaccine should be administered to children under five in high-endemic areas, while the use of LLINs remains an issue in certain regions. Coverage and usage rates will always differ. However, as mentioned in the Executive Director’s report, the funding for vaccines is not exchangeable with something else and is entirely separate. Trade-offs are allowed across other tools. So, the debate will continue.
Summary of Constituency Demands
Upper-Middle-Income Countries expressed concerns about reductions in allocations potentially impacting the sustainability of programs and reversing progress. Emphasis on the need for transition support and strategies to maintain gains made. While Key Populations wanted commitment that ensuring funding reaches marginalized and high-risk groups remains a priority and called for allocation methodologies to reflect the needs of key populations and address disparities across the board. What was repeatedly underlined was the need for greater flexibility to countries to decide the warp and weave of allocation. It is countries that need to have the agility to reallocate resources so that it could fulfil the mandate of reaching key populations speaking to their specific contexts. It was urged that there be recognition that a one-size-fits-all approaches are not effective.
The reasons for the above points of concern are detailed below
Programming Costing
The marked “inertia” in shifting the status-quo was remarked upon by stakeholders who seem to have run out of patience at the obduracy of the Global Fund in bringing the GDS to more closely align with the epidemiological evidence as was repeatedly recommended in the previous external review and which was rejected at the time as the Global Fund insisted other factors are also in play, besides epidemiological ones. But this is not convincing anybody. At the 51st Board meet, the Global Fund had mentioned cost of programming, among a host of other factors as the reason for not considering epidemiology as the sole factor for the GDS. But it is this very factor of Cost of Essential Programming (CoEP) that came under sharp scrutiny from constituents at the 52nd Board meeting.
There was appreciation that the GDS does enable higher allocation for TB and malaria and that countries have flexibility to align their indicative splits based on their epidemiological landscapes to ensure higher allocations for drug-resistant TB and insecticide-resistant vectors are prevalent. However, it was pointed out that in certain regions where the malaria burden has fallen, for instance, the intervention costs to sustain the program continue to remain high. And there were lots of questions on how CoEP has been calculated, its role in determining the GDS modifications as well as grant allocations. A constituency pointed out that there is a blanket assumption that all the allocated funds for the CoEP are being utilized optimally and no further efficiencies are necessary. There is also the glaring absence of what is to be done if the allocation amount based on the formula ends up being way higher than the CoEP. Moreover, countries from regions that do not fall within the Low-Income Countries bristled at the thought given that the proposed shift would mean that countries that are part of an entire constituency of the Global Fund would fall much lower than the CoEP level, even post-application of the mechanisms of the qualitative adjustments. Constituencies believe that the laser focus on allocation methodology, while understandable, ignores that qualitative adjustments also mean improving efficiency or diverting non-essential expenditure for better use of the monies where it’s more needed and must take into account a detailed assessment of challenging operating agent environment’s unique needs.
Country Economic Capacity
It was pointed out that the Board retreat in July 2024 had asked for a shift in the Country Economic Capacity (CEC) curve only in a scenario of low replenishment outcome in GC8 and yet, has been uniformly applied across all replenishment outcomes. This should be done only after a clear analysis on impacts and risks of the proposed shift. Moreover, shifting the CEC curve benefitting the low-income countries is fine but countries, which have attained gains need support to sustain them and ensure there are no reversals in the same. The minimum allocation of $500,000 that the Global Fund offered as a sweetener to brace against the impact of the CEC curve shift was not sufficient to assuage the countries in upper income level, who called for a case-to-case approach to determine the adequacy of the amount for sustaining essential programming, given the concentration of key populations. There is also need to ensure that the methodology for the CEC evolves to incorporate dynamic factors of climate change and conflict in regions beset by them so as to ensure real-time health needs of these regions are funded for. Examples cited were of measuring economic fragility, and proportion of refugees due to population displacement.
There is also no clarity on whether or not the Emergency Fund can be invoked in scenarios where the disease incidence is vaulting and when funding approved by the Global Fund gets stuck in red-tape at the country government level. This was the case when the HIV crisis hit Fiji in the early months of 2024, for instance.
Catalytic Investments
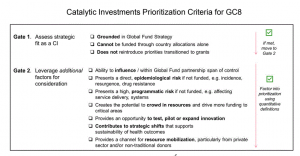
Catalytic priorities for 2026-2028 allocation period (Grant Cycle 8),
based on the total amount of sources of funds for allocation
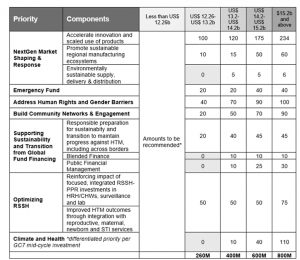
There was consensus that Catalytic Investments should be allowed only for urgent and impactful intervention not covered by existing country allocation and the proposed increased catalytic investment for upholding human rights and dismantling gender barriers was welcomed. It was underlined that allocation is not guaranteed unless a country is deemed eligible for it and countries need to prepare domestic sources of financing so as to sustain their programs rather than depend on the Global Fund. More clarity was sought by constituencies on how countries could effectively engage in private and alternate funding resource-sharing initiatives.
It was emphasized that there is an urgent need to maximize the usage of scarce resources and that catalytic investments will be of even more relevance in the event of lower replenishment. They will be critical for key populations and need to be protected in any scenario, and cover multi-country grants and for building community engagement and AGYW. Moreover, funds for building resilient and sustainable health systems need to be optimized and greater clarity is needed regarding the amount that will actually be spent towards community engagement, civil society and strengthening of the Country Coordinating Mechanism (CCM).
The Secretariat stated that catalytic investments will also be recommended to the Board in the event that the funding sources for allocation for the eighth grant cycle falls beneath $12.26 billion. However, serious reservations were expressed about catalytic investments diverting funds away from critical disease prevention and addressal of interventions in country grants within a low investment context. It was pointed out that there are large unfunded gaps in GC7 vis-à-vis the HIV, TB, and malaria country grants and CoEP calculations have not taken into account, for instance, that the highest proportion of critical gaps being in essential TB services. Stats were cited: every year 7 million people with TB do not have access to WHO-recommended TB diagnostics. So also, testing and treatment with antiretrovirals (ARVs) for nearly 7 million people living with HIV has also not been considered. And across all malaria countries the net gap equates to 238 million nets, which is estimated to leave more than 400 million people without this vital protection. Hence, it was highly recommended by constituencies to consider using only additional private funding for catalytic investments rather than dipping into funds meant for country allocations and setting these aside for catalytic investments in scenarios below GC7 level.
Conclusion
As pointed out in our article on the Global Fund’s upcoming 8th replenishment cycle, the Global Fund is the only global health initiative heavily dependent on US funding and has implications as our articles on the undue U$ influence on global HIV and Sexual Reproductive Health and rights and Reporting on the Results of the Global Fund – What’s missing? showed. The Global Fund is a public-private partnership. The contribution of the U.S. government plays a critical part in the funds at its disposal. In the Grant Cycle 7, the Global Fund aimed at raising $18 billion but could manage only $15.7 billion, still a record-breaking amount but falling way short of the target. As reported by Andrew Green in Devex, the U.S. adds to the coffers of the Global Fund. However, a law makes it binding on the government to provide up to a third of the total amount raised by the Global Fund from donors. But, the Global Fund could not fulfil the target amount so as to claim the full pledge under the U.S. law. And what it resulted in, pointed out Green, is that the Global Fund did not get the share it expected while UNICEF and Gavi, the Vaccine Alliance got more or less the same allocation from the U.S. that they did in 2023. To note, however, that on the face of it, this is more than what the Global Fund gets in its kitty. And the whopping increase of 23.9% from 2023 went to the WHO. This, despite a delegation of private donors calling on the United States Congress to prioritize strong investment in the Global Fund and lauding bipartisan congressional leadership support for the Global Fund. Since then, Trump has declared withdrawal from the WHO, which is to be confirmed. This has sent jitters through global health initiatives, wondering what is in store for them and this includes the Global Fund.
Hence, it is not surprising that the 52nd Board meet underscored the intricate balance required in allocating limited global health resources amidst evolving challenges. There is a collective understanding that achieving the ambitious targets set for HIV, TB and malaria will require sustained effort, increased funding, and innovative approaches. The commitment to adapt and respond to changing needs and contexts remains strong. Participants emphasized the importance of remembering the human impact behind the numbers—each allocation decision affects lives and communities worldwide. Participants expressed gratitude for the thorough analyses, technical expertise, and collaborative efforts that informed the decisions. While recognizing that the adjustments may not fully satisfy all stakeholders, they represent a strategic approach aimed at maximizing impact with the resources available.
As the meeting concluded, there was a renewed call to action:
- For Donors and Partners: To advocate for and secure increased funding, recognizing the profound impact additional resources can have.
- For Implementing Countries: To utilize allocations effectively, prioritize interventions with the greatest impact, and continue to strengthen health systems.
- For All Stakeholders: To maintain open communication, collaborate across sectors, and keep the focus on the ultimate goal—ending HIV, TB and malaria as public health threats.
The meeting served as a reminder of the progress made to date and the challenges that lie ahead. With a shared vision and concerted efforts, participants expressed optimism that the global community can overcome these challenges and achieve lasting health improvements for all.
Key Outcomes of the 52nd Board Meeting
Total Allocation: The meeting confirmed that $12 billion is designated for country allocations. This figure is based on detailed estimates of the essential programming costs required to address each disease effectively.
Data-Driven Decision-Making: Emphasis on using robust data and evidence to inform allocation decisions and regular updates and reviews to ensure allocations remain aligned with current needs and trends.
Methodology Review: A commitment was made to regularly review and update the allocation methodology every three years. This ensures the approach remains aligned with the evolving health landscape and maximizes the impact of available resources.
The strategy committee will conduct additional sessions in the coming year to further refine allocation methodologies and will consider new data, emerging health challenges, and feedback from stakeholders.
Catalytic Investments:
Discussions highlighted the critical role of catalytic investments in driving innovation and addressing systemic challenges and the imperative of balancing country allocations with funds reserved for catalytic initiatives.
Advocacy for Increased Funding:
Acknowledgment that achieving health targets requires increased global health funding and a commitment to collective advocacy efforts to secure additional resources.
Decisions Approved at the 52nd Board Meeting
- Allocation methodology, including its global disease split is approved.
- The SC is tasked to review and approve, in 2025, the method by which the Secretariat will apply and report on the qualitative adjustment process; and
- The Allocation Methodology and Technical Parameters shall apply for Grant Cycle 8 and supersede the 2023 – 2025 allocation methodology and technical parameters.
