Global Fund Allocation – A Brave New Method in the Offing?
Author:
Madhuri Kamat
Article Type:Article Number: 10
The Global Fund is under pressure to enhance the share of allocation for tuberculosis and malaria and also provide more for health system strengthening. These are the key issues that the Board had to decide even as an evaluation report and the Secretariat struggled to come up with answers. The Board made far reaching suggestions including a relook at the methodology of the Global Disease Split and actions to be taken going forward. Will things pan out as planned?
Allocation – What is it?
Allocation stems from the disease focus of the Global Fund, which uniquely remains only on HIV, Tuberculosis and Malaria, which has now become known by its short-form – HTM. The impact of the Global Fund depends largely on the amount of money in its kitty, which are the country allocations. Every country, regardless of whether they are donor or implementor countries, provide some largesse of their own. In addition to the country allocations, the Global Fund uses what it calls Catalytic Investments, to inject much-needed funding in priority areas that may not be adequately covered under the country allocations. As per Global Fund-provided data, “for the 2023-2025 allocation period, the Global Fund Board approved a total of US$13.128 billion for country allocations and US$400 million for catalytic investments.”
Figure 1: Overview of Global Fund 2023-2025 Allocation Methodology
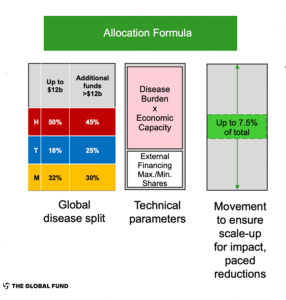
However, in recent times, the Global Disease Split (GDS) that is at the core of the Global Fund (Figure 1) came under intense review for two reasons: Firstly, on whether to add one more component of Resilient and Sustainable Systems for Health to HTM; and secondly, the need for tuberculosis and malaria to get an enhanced share of the disease split funding. This has already been undertaken under GC7, but there are calls to do more.
These issues were part of the review of the Allocation Methodology for the Global Fund Grant Cycle 8 (GC8). Following the report, the Secretariat also came out with its response. In this article, we provide some of the details of the 2023 report on the Review of Allocation Methodology for Grant Cycle 8 as well as the responses of the Secretariat to it. We also provide the discussions that took place on both during the 51st Global Fund Board Meeting in Geneva on April 24, 2024.
Review of Allocation Methodology for Grant Cycle 8
Excerpts from Review Recommendations & Secretariat Management Response
Global Disease Split (GDS)
Recommendation: to adjust the current GDS to better reflect the epidemiological situation and re-balance the distribution of funding across the three diseases to give more weight to TB based on the share of Disability-Adjusted Life Years (DALYs) and deaths.
Agree
The Secretariat agrees with the need to increase funding for TB. For this reason, the Board decided to increase the split for TB in GC7 for available funds for country allocation above US$ 12 billion.
Disagree
Reasons: The epidemiological landscape is [not] the sole factor that should determine the disease split, noting other factors are also important to consider, including the financing landscape, economic capacity, the cost of essential programming, previous funding levels, and the impact of investments.
Finally, DALYs will continue to be one piece of information to inform the review, however the Secretariat also does not agree with applying directly the share of DALYs proposed, due to the methodological limitations of using DALYs for resource allocation.
Recommendation: To protect the continuity of services, gradually changing the GDS over multiple allocation cycles to ultimately bring the entire split closer to the distribution by disease burden.
Agree but conditional
Any changes to the GDS cannot apply to all funding levels.
The Secretariat will include explicit consideration of revising the disease split as a part of each allocation cycle review but notes that a revision cannot be guaranteed, given the multiple factors to consider and the changing contexts over time.
Resilient and Sustainable Systems for Health (RSSH)
The evaluation concludes that creating a fourth share for RSSH in the upfront split is not recommended.
Agree.
As this will create a siloed approach, reduce funding for HTM in flat and lower funding scenarios, which could threaten life-saving interventions.
Disagrees that the expected advantage of an RSSH allocation is to increase RSSH investments.
Reasons: RSSH investments may decrease for some countries, depending on the intent and the parameters applied.
Accepted for consideration to improve the impact of RSSH investments in GC8:
Dedicating a set percentage or percentage range of each country’s allocation to RSSH, tailored to country context, with the percentage “calculated based on ad hoc qualitative analyses outside of the Allocation Methodology process.” Allocation letters to include the type of investments to be funded in each country “by level of priority”.
Disagree.
Reasons: it is not clear whether this percentage is to be communicated as a requirement or a recommendation. Other related decisions for consideration not mentioned in the report is how much program split flexibility countries will have to shift funds between RSSH and HIV, TB and malaria (HTM).
Noting the complexity of the issue and recommendation against adopting a fourth split for RSSH in the allocation methodology, the Secretariat will consider all additional levers to address the identified challenges to delivering impact on RSSH and propose options for discussion to the Strategy Committee and Board
Technical Parameters
The Secretariat does not agree with the evaluation’s recommendations related to the technical parameters as stated below.
Gross National Income
The evaluation notes, “GNI per capita is the best primary indicator for country economic capacity.” Considering government revenue per capita and other fiscal capacity indicators in the qualitative adjustments, rather than formulaically was also recommended by an externally commissioned 2021 review on economic capacity in the Eligibility Policy and Allocation Methodology.
Recommendation: “potential consideration” to complement GNI per capita with a public revenue per capita, adjusted for public or publicly guaranteed (PPG) debt interests.
Disagree.
Reasons: In terms of data availability, government revenue per capita data is available for a limited number of countries (as the evaluation notes) or would have to be constructed (as it is available more widely from the IMF in national currency).
The evaluation’s proposal to collect the data from Country Coordinating Mechanisms (CCMs) is not only more challenging than the evaluation implies, it would also lack the necessary rigor and comparability for inclusion in the formula.
Finally, the proposed two-stage approach – introducing these indicators in the qualitative adjustments for GC8 and then in the formula the following cycle – would not overcome the above limitations of including these indicators in the formula
As in the past two cycles, the Secretariat will review economic and fiscal capacity indicators in preparation for the GC8 qualitative adjustments factors and process, which will come to the Strategy Committee for decision in 2025.
Inclusion of Country Performance Indicators
Recommendation – adding a composite index on government effectiveness
Disagree.
Reasons: analysis provided in the evaluation shows weak correlation between the performance indicator used (average Country Performance Rating from the World Bank’s IDA allocation formula) and the prevalence of the three diseases;
Country Performance Rating is based on a qualitative country policy and institutional assessment.
The second performance indicator proposed – to capture government prioritization of health spending – is already factored in the determination of the co-financing incentive.
Inclusion of Vulnerability Indicator
Recommendation: “potential consideration” to add a vulnerability indicator to the allocation methodology.
Disagree.
Reasons: While recognizing the importance of accounting for vulnerability in the Allocation Methodology, would only add a vulnerability indicator to the Allocation Methodology – whether in the allocation formula or the qualitative adjustments – if there is a well-defined need and a clear incremental benefit.
Several dimensions of vulnerability are already reflected in the outcome of the allocation methodology – for example, 71% of the GC7 allocations went to the 50 most climate vulnerable countries.
Cyclical Review process
The Secretariat recognizes the finding that Strategy Committee and Board members raised the need for a more holistic view on the Allocation Methodology decision-making process. Will consider it in the preparation for the GC8 Allocation Methodology process.
Certain decisions are required early to inform subsequent steps and related processes. For example, the GDS decision informs the design of the next steps of the Allocation Methodology.
Catalytic Investments
No modification required. Agree.
Recommendation: the catalytic results from previous cycles be aggregated to inform the total catalytic funding envelope.
Disagree: the catalytic modalities (Strategic Initiatives, Matching Funds and Catalytic Multi Country) are very different in nature. Catalytic priorities may change between cycles to respond to the evolving context or a new Strategy.
Limitations of the Evaluation Report of the Allocation Methodology – Excerpt
The Secretariat notes that many of the recommendations lack specificity about the associated trade-offs and their operationalization.
The Secretariat also observes a number of limitations related to the conducted analyses.
Example: much of the analysis for the Global Disease Split replicates what the Secretariat did for the last global disease split review for GC7 (e.g. share of DALYs and deaths, disease funding by income), which led to the revised Global Disease Split for GC7.
CCM survey findings are presented by respondent rather than country. While this bias was taken into account at the start of the report, it is not discussed or reflected clearly when the survey results are used and presented in the findings.
The report includes an overview of the allocation methodologies of Gavi, the Vaccine Alliance, the Global Financing Facility (GFF) and the World Bank’s International Development Association (IDA), but lacks an assessment of how the lessons learned would be applicable to the Global Fund’s operational context and how they could inform the Global Fund’s Allocation Methodology.
Gaps
The Secretariat was looking for clear answers to the pending issues of inclusion of RSSH and increase in the GDS vis-à-vis TB and malaria. While it did get a clear response on the former, the latter remains up for debate because as the Secretariat pointed out, “the evaluation does not include a recommendation on where the increased share for TB should come from, which limits its utility”. And although there was agreement that the changed epidemiological and external financing landscape suggests “a revised split in favor of malaria (as well as TB) and away from HIV, this was not reflected in the recommendations. In addition, the assessment lacked specificity as to how the split should change and the associated implications.”
The Independent Evaluation Panel (IEP) endorsed the evaluation because the assessment tool against which it was scored was put in place only after the evaluation was completed. Hence, the IEP chose to highlight some of its shortcomings, which included weaknesses in the methodology and framework of the evaluation though it found the overall quality was satisfactory. The IEP also felt it was useful in its analysis of forward-looking alternatives and their implications and had responded to all questions.
Stakeholder Feedback
Modifying the Global Disease Split – Stop TB Partnership Weighs In
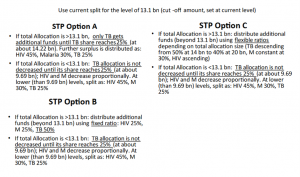
The Stop TB Partnership in the run-up to the Board meeting made suggestions on the options for the Global Disease Split (Figure 2) without having to decrease the allocations for HIV or malaria, while also ensuring that Low-Income Countries and Africa, will not suffer.
Figure 2: Global Disease Split Options – Stop TB Partnership Stakeholders Feedback
Discussions on Allocation Methodology
Stakeholders cautioned for the need for assessing potential inimical effects of a disease rebound, especially for the most affected and vulnerable populations in the event of a premature Global Fund transition. Catalytic investments such as Multi-country Grants were lauded for ensuring that cross-border issues that get overlooked during country-specific approaches get addressed and facilitate the strengthening of a targeted, customized approach for those most in need and affected by the three diseases.
Besides Gross National Income as an indicator of economic capacity, public revenue per capita was suggested as an additional indicator along with other criteria such as budget analysis, tax revenue, debt burden, and annual interest payments as well as principles that influence effectiveness, efficiency and flexibility for countries. It was also pointed out that Upper Middle-Income countries and small economies facing climate change threats are not being considered when determining GNI as the sole criteria of a country’s economic status. There were also calls for more inclusive consultations that included all key populations and civil society while discussing the revision of the allocation methodology and to allow and respect country priorities and country ownership in determining RSSH investments.
The Board Responds
The Board also expressed frustration at the evaluation failing to address critical political and policy-related questions, something which was highlighted by the IEP. The feedback highlighted the ongoing need to refine the Global Disease Split, considering new economic data and the realities of countries heavily reliant on global financing. The Secretariat acknowledged the importance of incorporating a principled approach to the GDS, considering both quantitative and qualitative adjustments to better reflect the economic capacities and specific health financing needs of countries. After many questions about the Allocation Methodology and long hours of discussion spent to identify areas requiring immediate attention and potential refinement, recommendations emerged from the Board so as to ensure that the allocation methodology remains robust, equitable, and adaptive to the ever-changing landscape of global health needs.
Recommendations
- Evaluations of Allocation Methodology:
Future evaluations need to be more encompassing, offering clear pathways and alternatives rather than merely reiterating existing data.
- Action: Future evaluations should be structured to provide actionable insights and clear, political and policy-aware recommendations that guide decision-making at all levels.
- Alternatives to Global Disease Split:
Need for a transformative approach that could better balance the fund distribution reflective of disease burden and associated treatment costs. Members advocate for an initiative to explore and develop new models that are data-driven and capable of adapting to the dynamics of global health challenges.
- Action: Establishment of a task force to develop new frameworks for the global disease split, ensuring that these are informed by comprehensive data analysis and reflect true needs.
- Procedural Aspects of Funding Allocation:
Continuation of guidance through the entire funding phase, including country dialogues for ensuring consistency and effectiveness in the implementation of funded projects. More structured follow-through in future allocation cycles to prevent discrepancies and enhance the impact of funding.
- Action: Continue to refine the processes surrounding funding requests and country dialogues to ensure they are strategically aligned with both global health objectives and country-specific needs.
- Integration of COVID-19 related investments into the allocation framework:
It is necessary to devise strategies that allow these investments to extend beyond the current endpoint of December 2025. This reflects an understanding of the long-term impacts of the pandemic and the need for sustained support in response efforts.
- Action: Plans for the strategic integration of COVID-19 investments should be detailed and forward-looking, ensuring they align with broader health system strengthening and pandemic preparedness.
- Emergency Funding Mechanisms:
These mechanisms are crucial for maintaining flexibility and responsiveness within the funding model to address unexpected health emergencies in participating countries.
- Action: Expand and refine emergency funding mechanisms. Including simulated funding releases during mid-cycles to provide more robust support for countries facing sudden health crises, ensuring these mechanisms are adaptable and responsive.
- Catalytic Funding:
Catalytic funding, although not part of the evaluation session, was recognized as a critical component of the overall funding strategy.
- Action: Holistic Integration of Catalytic Funding, ensuring it complements and enhances the strategic objectives across all funding allocations and health initiatives.
- Economic variances across different countries and their implications for fund allocation:
More nuanced and balanced approach to economic factors in fund allocation, stressing the importance of maintaining a focus on populations and regions with the greatest needs.
- Action: As economic scenarios evolve globally, the allocation methodologies need to be flexible yet targeted, ensuring equitable access to resources for all countries, especially those less able to generate health funding domestically.
Conclusion
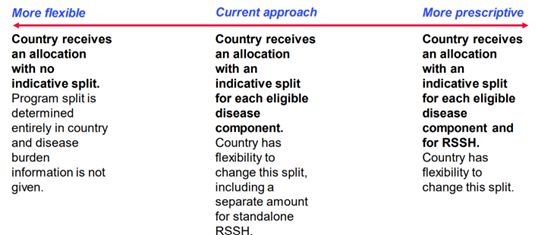
The discussions have set the stage for significant enhancements in how health funding is allocated and managed. Now it remains to be seen how things work out in the coming period of the Grant Cycle 8 (Figure 3 and 4) as the recommendations are acted upon. A lot will depend on the proposed Task Force on the Global Disease Split.
Figure 3: Global Fund-proposed Focus Areas for Allocation Methodology in GC8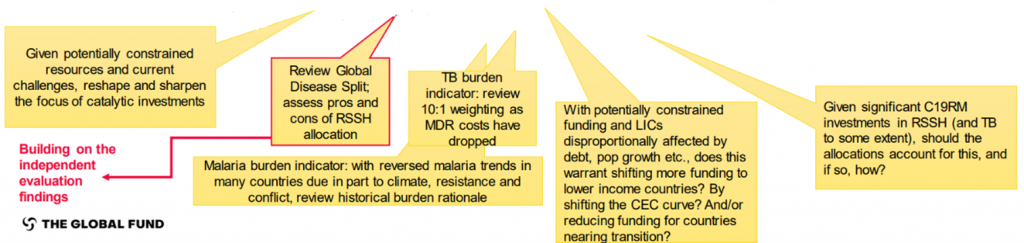
Figure 4: Country Ownership: Which way to go in Allocation?