
HIV: healing a minority in a world of inequalities?
Author:
Ekelru Jessica and Christian Djoko
Article Type:Article Number: 7
This article aims to demonstrate that, despite the excitement generated by the announcement of the seventh patient cured of HIV, the pandemic remains a global crisis of considerable proportions, affecting more than 39.9 million people, nearly 10 million of whom are deprived of access to care. Inequalities, aggravated by stigmatization, particularly affect marginalized populations. The article calls for the strengthening of community-based approaches for a more equitable fight against HIV, while stressing the importance of accessible scientific progress and the fight against structural inequalities in eradicating the disease.
Introduction
At the AIDS 2024 conference, sensational news was announced: the definitive cure of HIV in a seventh patient, dubbed the “Berlin patient”. This announcement, while marking a major milestone in scientific research, was accompanied by a disproportionate media hype that could be misleading as to the current state of the HIV pandemic. It is essential to understand the real significance of this breakthrough, and not to lose sight of the continuing challenges in the fight against HIV.
A scientific breakthrough with limited applications
The cure of HIV in this seventh patient relies on highly specialized medical interventions, such as stem cell transplants combined with extremely strict immunosuppression protocols. While these methods are remarkably effective in individual cases, their complexity makes them difficult to apply on a large scale. Indeed, these procedures require advanced medical infrastructures, massive financial resources and specialized clinical expertise. What’s more, they carry considerable risks for patients, further limiting their broader applicability
Stem cell transplants, based on rare genetic compatibility, are the privilege of a few, a luxury reserved for very specific contexts far removed from the realities of poor or developing countries. These operations require prolonged periods of hospitalization and rigorous medical monitoring to prevent graft rejection and treat opportunistic infections linked to immunosuppression. Such constraints make these treatments inaccessible to the vast majority of people living with HIV (PLHIV), particularly in hard-hit regions such as sub-Saharan Africa, where medical resources are limited and health systems under pressure.
The HIV pandemic: an ever-present crisis
In fact, individual successes, such as the “Berlin Patient” cure, must not obscure the crying need for prevention, treatment and ongoing care. The HIV pandemic remains a colossal challenge that transcends borders, a persistent crisis affecting more than 39.9 million people worldwide (Figure 1), with an alarming proportion of almost 10 million people lacking access to the necessary treatment. In 2023, one person died of HIV every minute, a figure that sounds like a cry of despair in a world where scientific advances are not reaching all people, especially those on the margins of the global economy.
In Africa in particular, where economic, geographical and social inequalities limit access to healthcare, the challenges are particularly acute. Health infrastructures are often inadequate, preventing millions of people from accessing life-saving treatments, and perpetuating HIV-related suffering and mortality. Treatment is still a privilege, not a universal right. The paradox is clear: we celebrate spectacular advances in privileged contexts, while millions of people continue to suffer and die in the world’s relative indifference.
Figure 1: Regional data for 2023
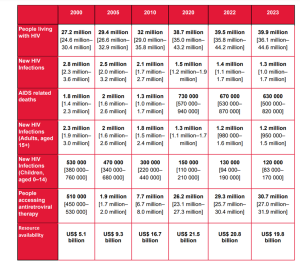
Source: UNAIDS epidemiological estimates, 2024.
Inequality of access to care is already a cause for concern for many PLHIV, and is exacerbated by stigmatization and discrimination. This stigma, whether social, institutional or gender-based, continues to reinforce barriers to accessing care. Marginalized individuals, including women, children and key populations such as sex workers, transgender people, men who have sex with men and injecting drug users, are the hardest hit by these inequalities. These populations, already vulnerable because of their social position and marginalization, suffer a double penalty, both as victims of a global epidemic and as targets of institutionalized discrimination that excludes them from healthcare systems.
Difficult access to healthcare is not just a question of medical infrastructure, but is also rooted in social, economic and cultural factors. Limited access to education and health information, economic insecurity, as well as social and legal norms that perpetuate stigma and discrimination against key populations, reinforce these obstacles. According to the West Africa regional report of the (p. 25), out of a sample of 10,910 people living with HIV (PLHIV), here are the percentages, by category, of those who said they had avoided going to a health center for care in the last 12 months because of their HIV status.
| Category | Percentage who avoided health centers |
|
Total PHAs |
7,5 % |
|
Key populations |
11,6 % |
|
General population |
6,2 % |
|
Transgender women |
17,5 % |
|
People aged 18-24 |
12,7 % |
|
People over 50 |
6,9 % |
|
Drug users (n=76) |
17,5 % |
|
Transgender people (n=123) |
14,9 % |
Thus, women and girls, especially in contexts of high economic dependence and low empowerment, are particularly vulnerable to unequal treatment in healthcare services. Similarly, men who have sex with men and transgender people often face institutionalized discrimination, resulting in denial or limited access to healthcare, as well as violence and further marginalization.
Figure 2: An overview of differentiated inequalities and vulnerabilities
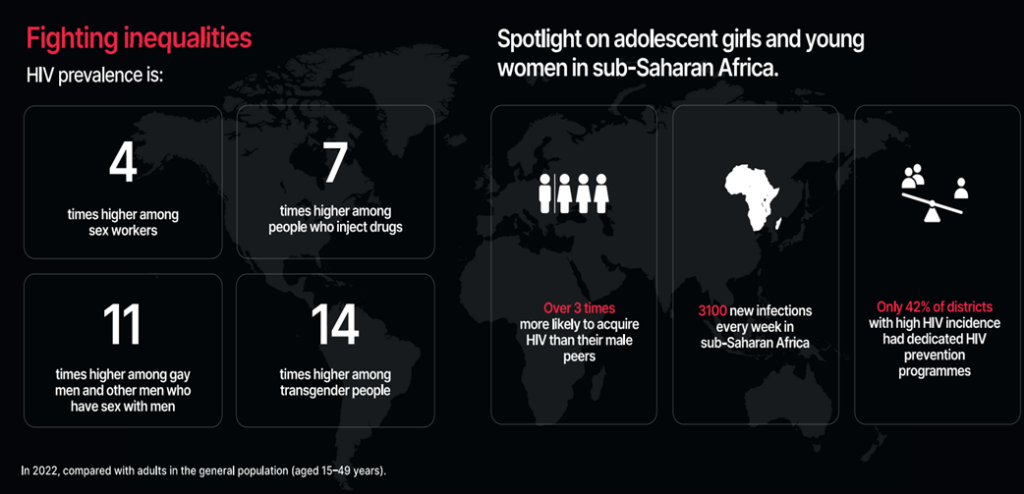
Source: UNAIDS
Faced with this reality, it is more essential than ever to strengthen activist and community-based approaches in the fight against HIV, with a resolute focus on equity and human rights.
Towards a realistic and inclusive approach to the fight against HIV
Announcements of cures, however spectacular, must be received with caution and communicated in a way that reflects their limited short-term impact. The eradication of HIV will only be possible when these discoveries can be replicated on a large scale and made accessible to all people living with the virus, whatever their geographical or socio-economic situation. In the meantime, strengthening activist and community-based approaches, with a focus on equity and human rights, is not only an effective health strategy, but also a moral and political imperative to ensure a truly inclusive and just fight against HIV.
Indeed, militant mobilization remains an indispensable lever for influencing public policies and demanding sufficient funding, while promoting an equitable redistribution of health resources. Community-based approaches, meanwhile, are vital for anchoring the response in local realities, where the trust and commitment of peers are crucial to reducing stigmatization and strengthening access to services. These initiatives are vectors of empowerment, enabling those most affected by the epidemic to become key players in the design and implementation of interventions. A resolute focus on equity also means recognizing and addressing the multiple forms of discrimination that are holding back progress: whether it’s the rights of women, sex workers, LGBTIQ+ people or drug users, the fight against HIV must inevitably go hand in hand with the fight for human rights.
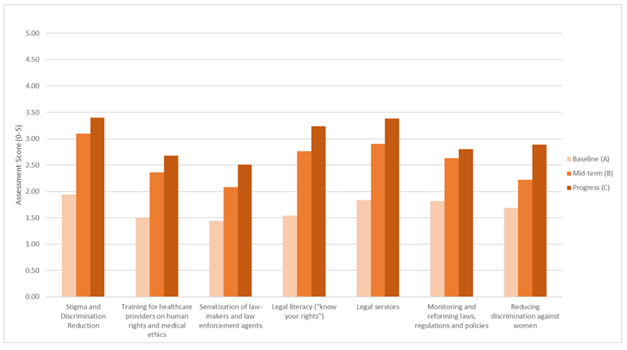
The initial results of the “Raise the Barriers” initiative, launched in 2017 by the Global Fund, accredit the approach advocated above. This initiative, which provides technical and financial support to 24 countries, aims to eliminate human rights and gender-related barriers impeding access to HIV, tuberculosis and malaria services. Although the implementation of comprehensive programs has been complex, the results convincingly demonstrate what can be achieved with continued investment and sustained effort. The most notable progress was made in the initial phase, between the baseline and mid-term assessments, reflecting the momentum of the first interventions. However, from the mid-point onwards, the pace of progress slowed somewhat, which was to be expected, not least because of the challenges associated with the final stage of interventions (Figure 3). This underlines the importance of strengthening resources, time allocation and commitment in order to extend the geographic and demographic reach of programs, particularly in a context like Africa where advocacy remains crucial.
Figure 3: Average scale of programs to remove human rights barriers to HIV by program area.
More broadly, a focus on equity requires an intersectional approach, which recognizes that factors of vulnerability to HIV are superimposed on other forms of marginalization (gender, sexuality, socio-economic status, access to education, etc.). In Africa, where gender disparities and systemic violence continue to limit women’s access to health services, it is crucial that community-based approaches advocate for genuine equality of treatment and a reduction in structural inequalities. Far from being a purely technical or logistical issue, the fight against HIV must therefore be seen as a political and social struggle, whose success depends on the ability to challenge the hierarchies of power that underpin health inequalities.
Conclusion
The announcement of the cure of the seventh HIV patient is an impressive scientific breakthrough, but it must not mask the profound realities of injustice and inequality that persist in the fight against HIV/AIDS. While this announcement brings hope, it is crucial to maintain a realistic perspective on its overall impact. The HIV pandemic remains a public health crisis of unprecedented gravity, requiring a collective, sustained and inclusive response.
Future scientific advances will need to focus on accessibility and large-scale replication to turn the hope of a cure into a reality for everyone. In the meantime, it is imperative to continue to intensify efforts to expand access to existing treatments and support the most affected populations. HIV eradication is a long-term goal, but it can be achieved if we remain committed, invest sustainably in public health and adopt an inclusive and equitable approach. Only by combining scientific progress, political will and humanitarian commitment can we one day hope to put an end to the HIV pandemic and guarantee an AIDS-free future for all. Herein lies the real promise of a universal cure.
