
A person currently dying of tuberculosis is murdered
Author:
Christian Djoko and Ekelru Jessica
Article Type:Article Number: 8
This article is an opinion piece designed to demonstrate that the eradication of tuberculosis is less and less a challenge to science than a problem linked to stigmatization and, above all, the under-funding of the response. Based on this observation, the text concludes that anyone dying today from this curable disease is simply a victim of non-assistance to a person in danger.
Tuberculosis (TB) is a deadly infectious disease that kills around 3,600 people every day, mainly in developing countries. Caused by the bacterium Mycobacterium tuberculosis, the disease has been rife for some 40,000 years and has evolved into a stubborn, resistant pathogen that is particularly difficult to eradicate.
In 2022, 10.6 million people contracted tuberculosis, and 1.5 million died from it, representing an average of 2.5 deaths per minute. These figures (Figure 1) underline the gravity of the situation: TB has regained its position as the world’s leading cause of infectious mortality, after a brief interlude due to the Covid-19 pandemic. In the few minutes it takes to read this article, some fifteen people will have succumbed to this disease.
Figure 1: Tuberculosis data worldwide in 2022
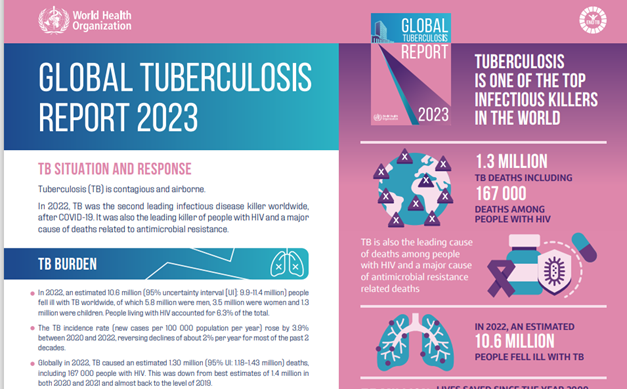
Source: WHO
It was in this context that we recently took part in the regional meeting entitled “Advancing community, rights and gender for an equitable response to TB in Francophone Africa”, organized by the Stop TB Partnership and Draft TB in Yaoundé, Cameroon, from June 11 to 13, 2024. (Read our article on the highlights of this meeting here). This meeting enabled us to witness once again the deep commitment of communities in the fight against this devastating disease.
These community players, mostly former patients, devote their lives to this cause with unshakeable determination. They invest their time and resources on a daily basis to integrate rights-, community- and gender-based approaches in the fight against tuberculosis. This dedication was particularly evident in discussions, workshops and intensive work sessions, such as those held in Yaoundé, where participants relentlessly exchanged ideas on how to improve the integration of these approaches into control strategies. This is essential to ensure an equitable and effective response.
What happened in Yaoundé is not an isolated case. In many countries of the Global South, similar initiatives are being undertaken, where entire communities are mobilizing against tuberculosis. As we consult existing documentation, action plans and available tools, or attend the many meetings, workshops and conferences dedicated to this cause, We’re always struck by the existence of a veritable community of practice. This community is made up of highly qualified and competent people, all united by a common goal: to put an end to tuberculosis.
On our return from the Yaoundé meeting, a slogan still comes to mind, a mantra repeated by the participants as a sort of rallying cry: “Yes, we can end tuberculosis”. This shared conviction, this slogan, full of hope and determination, led us to ask ourselves profound questions: what is really standing in the way of our efforts to eradicate this disease? What is preventing the elimination of a disease that we have long known how to treat and prevent? Why do so many people continue to die from a curable disease?
Although significant progress has been made in the fight against tuberculosis, as evidenced by the results achieved by the Global Fund in the countries in which it has invested since 2002 (Figure 2), the figures remain alarming and dramatic. It is a deadly divide (Figure 3), to borrow the title of an accountability report by tuberculosis-affected communities and civil society (Commitments vs. Realities).
Figure 2: Trends in tuberculosis deaths (excluding HIV-positive people) in countries where the Global Fund invests.
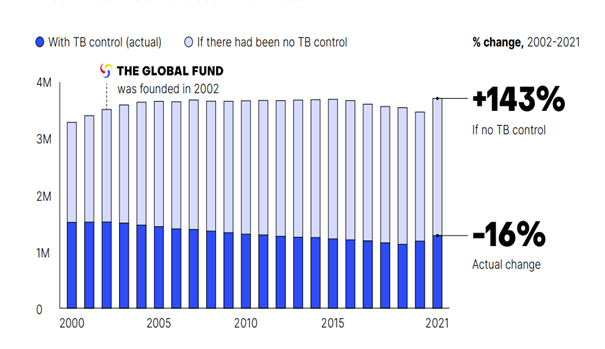
Source: Global Fund 2023 Results Report (p. 38)
Figure 3: Deaths attributable to tuberculosis: progress towards WHO target (in countries where the Global Fund invests)
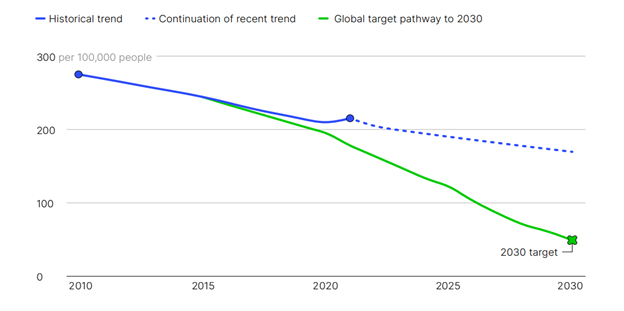
Source: Global Fund Results Report, (p.35)
This is all the more tragic given that we have the knowledge and tools to eradicate this devastating infectious disease.
Medical science has made remarkable advances in the prevention, diagnosis and treatment of tuberculosis. Effective drugs exist to cure the majority of cases, and preventive strategies such as BCG vaccination have proved effective in many cases. However, the implementation of these solutions remains insufficient. While we know what needs to be done to reverse the current incidence of tuberculosis and eradicate it as a public health problem by 2030, the efforts being made are still insufficient.
In fact, what we’re really trying to get you to understand is that every death from tuberculosis is preventable. In other words, there is good reason to believe that a person currently dying of tuberculosis is, in a way, a victim of negligent homicide. This is nothing less than non-assistance to a person in danger.
This situation is due to a number of factors, which the participants at the Yaoundé meeting described in detail. Among the many factors highlighted, at least two interdependent ones seemed to be common to all the countries represented: insufficient financial resources allocated to the fight against tuberculosis, and the persistent stigma associated with the disease.
Let us quickly remind you that, at the time of its seventh replenishment, the Global Fund needed at least 18 billion dollars (which was already far from the real needs) to fight tuberculosis, among other diseases (Figure 4). It raised only US$15.7 billion.
Figure 4: Overview of resource requirements and forecast of available resources for HIV, tuberculosis and malaria in countries where the Global Fund invests
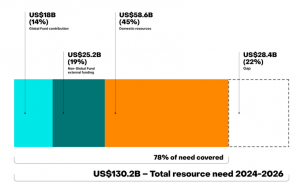
Source: Fighting for what matters. Investment pitch
Lack of financial resources, particularly in low- and middle-income countries, is a major obstacle to the fight against tuberculosis. This makes it impossible to mobilize or implement all the knowledge, tools and strategies needed to eradicate tuberculosis as a public health problem. Who is responsible for this situation? Rich countries, no doubt, although some of them are making a significant contribution to the fight against tuberculosis. However, the main responsibility lies with the countries of the Global South, particularly in Africa, which, despite numerous declarations, intentions and pompous resolutions, often taken at international meetings which for some delegations resemble pleasure trips, are not investing sufficiently in the fight against tuberculosis and, more generally, in the health sector.
For many governments, spending on the health sector is still seen as a cost, when it should be seen as an investment. Admittedly, these governments face many economic difficulties and budgetary tensions, but a comparison of health budgets with those of other ministries reveals that budgets are not just a column of numbers: they also reflect political choices. It’s more than obvious that the health of their populations is not yet a priority for many governments in the Global South. Yet, beyond the moral imperative of saving lives, money invested in health is also, and perhaps above all, an economically profitable investment for a country.
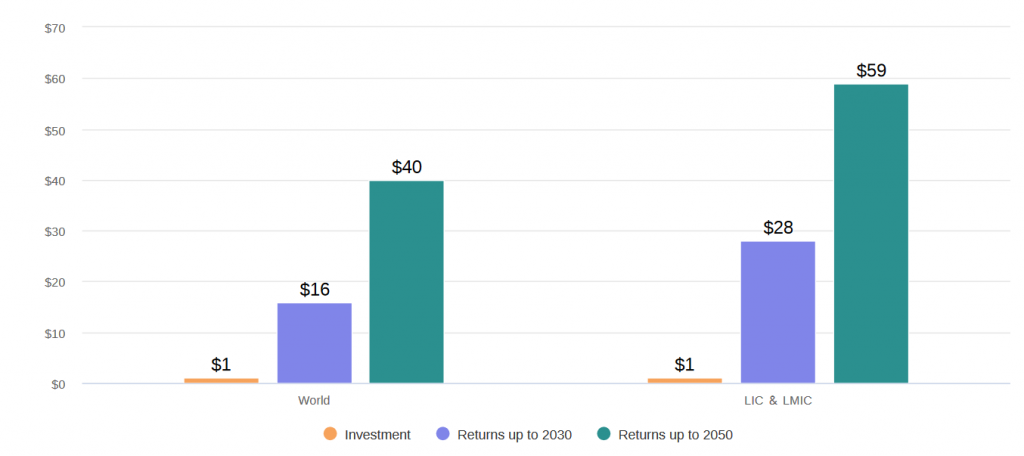
This is illustrated by a model (Figure 5) from Stop TB Partnership. For example, it predicts that “implementation of the global plan’s priority actions would generate an overall return of $40 for every dollar invested, and $59 for every dollar invested in low- and middle-income countries, with benefits accruing through 2050“. This analysis clearly demonstrates that investment in the fight against tuberculosis generates substantial long-term economic benefits, making any reluctance to allocate funds to this sector not only short-termist, but also economically irrational. Generally speaking, the price of inaction in healthcare is devastating in every respect, as demonstrated by a recent study published in BMJ journals.
Figure 5: Return on investment
 Source: Global Plan to Eliminate Tuberculosis (2023-2030)
Source: Global Plan to Eliminate Tuberculosis (2023-2030)
Beyond financial barriers, tuberculosis is also heavily affected by stigma and discrimination against sufferers. Fear of social exclusion, rejection and discrimination can dissuade individuals from undergoing screening and treatment, for fear of being marginalized or ostracized by their community. This stigma can also lead to self-medication and non-compliant treatment practices, which contribute to the worsening of the disease and the spread of antibiotic resistance.
Negative attitudes towards tuberculosis are often rooted in irrational fears and misconceptions about disease transmission. The association of tuberculosis with poverty, marginalization and risky behavior can fuel the stigmatization and social exclusion of those affected, particularly members of the LGBT community.
The Global Fund’s current scale of resource allocation (2023-2025) reveals that funds allocated to tuberculosis represent only a third of those devoted to HIV, and just over half of those dedicated to malaria (Figure 6). On a global scale, between 2002 and 2022, Global Fund investments in the three major diseases are distributed as follows: $27 billion for HIV, $9.5 billion for tuberculosis, and $16.2 billion for malaria. This distribution raises major concerns, even within the Global Fund, about the effectiveness of the fight against tuberculosis, especially when we consider the high incidence and devastating consequences of this disease in many parts of the world. As we write these lines, a discussion is underway at the Global Fund Strategy Committee meeting. The results of these deliberations will be known in the coming months.
Figure 6: Allocations by disease (in millions of US dollars)
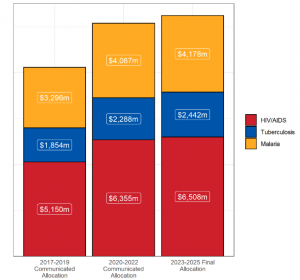
Source: Global Fund
In the meantime, it has to be said that the recurrent debate surrounding the revision of the resource allocation methodology has often focused on a re-balancing between these three diseases, with growing pressure to increase the share dedicated to the fight against tuberculosis. However, it seems to me more necessary than ever in the context of the forthcoming eighth grant cycle to break with traditional patterns of thinking. In other words, if we want to do what we’ve never done before, perhaps we should do what we’ve never done before. Let us explain.
Instead of getting bogged down in interminable debates about the distribution of resources between diseases, it seems more pertinent to first seek to substantially broaden the base of available resources. An illuminating analogy would be to compare this situation to a 14 cm pie or pizza. If the aim is to offer larger, more substantial portions to those who will consume it, redistributing the existing portions won’t fundamentally change anything. The solution lies in acquiring a larger pizza, 30 cm for example.
Let’s transpose this analogy to the context of Global Fund allocations: to increase resources dedicated to the fight against tuberculosis, we must first work collectively to increase overall funding for these diseases. This strategy will not only ensure adequate funding for the fight against HIV and malaria, but will also considerably strengthen efforts to combat tuberculosis.
Finally, allow us to share this projection (Figure 7) from the Stop TB Partnership on the financial resources needed to eradicate tuberculosis by 2030. Looking at these figures, one cannot help but be struck by the scale of the challenge ahead. Yet we have no choice but to continue fighting with determination to put a definitive end to this deadly disease. It’s in the interest of each and every one of us. The future of millions of lives depends on it.
Figure 7: Financial resources needed to end TB by 2030
Source: Global Plan to Eliminate Tuberculosis (2023-2030)
