
Global Fund Grants to the Republic of Niger
Author:
Oliver Campbell White
Article Type:Article Number: 4
Non-governmental principal recipients appear more capable at implementation
The Office of the Inspector General’s audit report on the Global Fund grants to Niger shows good performance of the charity-managed malaria program and improved availability of key health products. By contrast, there has been limited progress to improve HIV quality of care and data reporting and the low HIV and TB grants absorption rates suggest that grant activities are either partially or entirely not being implemented. It appears that more needs to be done to improve the grant absorption rate.
Background
On 28 March 2023 the Office of the Inspector General (OIG) published its report on the Global Fund grants to Niger which covered Principal Recipients (PRs) and Sub-Recipients of the Global Fund supported programs for the NFM2 and NFM3 grants from January 2019 to June 2022 (see Table A) but excluded TB diagnosis and treatment:
Table A: Principal Recipients and Sub-Recipients, Global Fund grants
|
Disease Component |
Principal Recipients |
Sub-Recipients |
||
|
Civil Society |
Public Sector |
|||
|
HIV / AIDS |
The Ministry of Public Health, Population and Social Affairs (MOH) |
PLAN Niger ONEN RENIP+ SONGES |
National AIDS and Hepatitis Control Program (PLNSH) |
|
|
Tuberculosis |
The Ministry of Public Health, Population and Social Affairs |
PLAN Niger ONEN |
National TB Control Program (PNLT) |
|
|
Malaria |
Catholic Relief Services (CRS) – United States Conference of Catholic Bishops (CRS (Niger) |
None |
National Malaria Control Program (PNLP) |
|
The Global Fund has classified Niger as a Challenging Operating Environment (COE) since 2016 because of its volatile political and security situation and it is also under the Additional Safeguard Policy for the past 10 years (see our article on the ASP here).
By way of background, the report notes that: (i) more than 4.4 million people became acutely food insecure during 2022, representing over 17% of the population; and about 6.8 million people are chronically food insecure; (ii) despite its continuous gross domestic product (GDP) growth since 2000, GDP contribution to health is relatively low (6% in 2019); and (iii) the country has a shortage of health workers with 0.04 physicians per 1,000 people against a World Health Organization (WHO) standard of one per 1,000 people.
As of September 2022, active grants totalled €153.50 million, of which 58% was disbursed for the 2021 to 2024 funding allocation period:
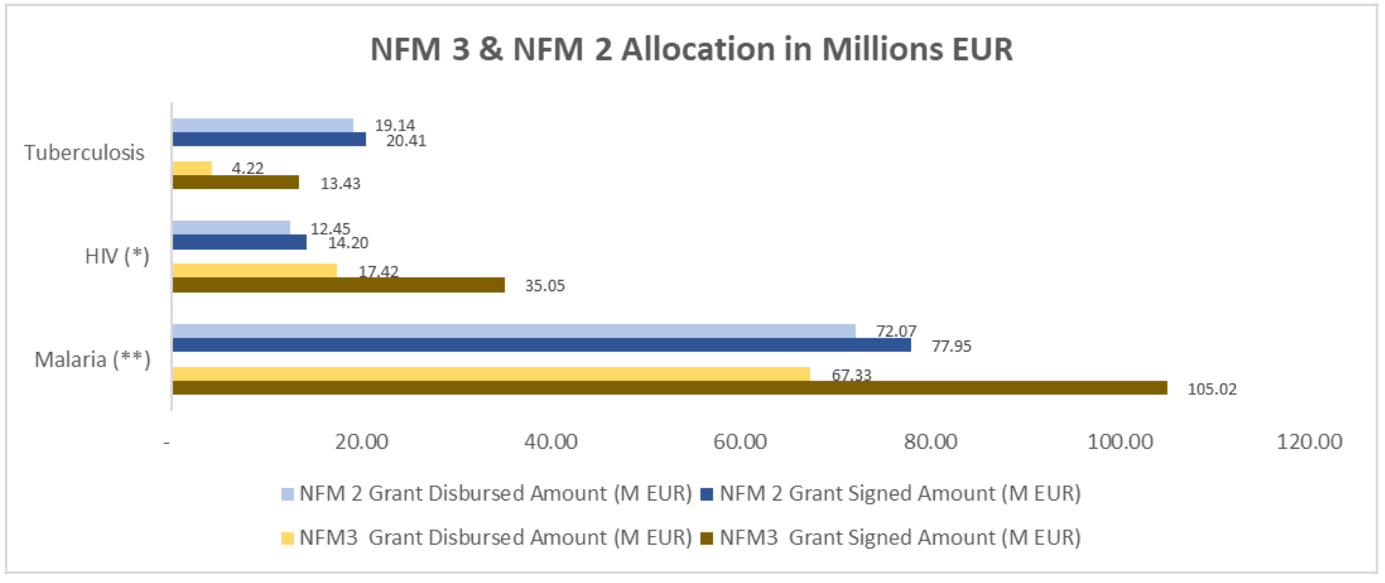
Note: The NFM3 TB grant started in 2022 so the amount shown is after one year of implementation; HIV and malaria disbursements are for two years of NFM3.
The report provides the following table (Table B) on the disease burdens up to end 2021:
Table B: Disease burdens in Niger, end 2021
|
HIV / AIDS |
Tuberculosis |
Malaria |
|
30,000 people were living with HIV as of 2021, of whom 81% knew their status and were on treatment. Annual new infections decreased by 17% from 1,200 in 2010 to 1,000 in 2021. AIDS-related deaths decreased by 54% from 2,200 in 2010 to 1,000 in 2021. Only 40% of pregnant women who tested HIV positive received ARVs in 2021. |
Of the 20,136 estimated TB cases, only 64% were notified. TB incidence has declined since 2010, from 191 to 79 per 100,000 people in 2021. Mortality rate has decreased since 2010, from 58 per 100,000 to 13 in 2021. Treatment success rate has remained close to the WHO target of 90% (84% of new TB cases in 2020 cohort).
|
Malaria is endemic across the country with peak transmission during the rainy season. WHO estimated 8.2m malaria cases in 2021 (vs 6.8m in 2010), with 3.2m cases treated with ACT (vs. 2.9m in 2018). Malaria rapid diagnosis test is the main method of confirmation with 5.6m tests carried out in 2021 against 1.6m in 2011. Estimated malaria-related deaths slightly decreased by 6%, from 26,471 in 2010 to 24,997 in 2021. |
First Finding
The first finding is that the good performance of malaria programs supported by the Global Fund over the past 10 years has helped to significantly decrease Niger’s malaria burden. However, to ensure improved impact of interventions in the next funding cycle, the surge in cases and deaths since 2017 needs to be investigated and adaptive measures considered for responding to challenges identified through the investigation.
From 2012 to 2021, incidence per 1,000 inhabitants decreased by 31% and the case fatality rate fell from 4.8% to 1.47% over the same period. These achievements reflected increased coverage for prevention and case management over time. However, despite this progress, confirmed and presumed malaria cases increased by 70% between 2017 and 2021 (from 2.8 million to 4.5 million). The number of severe malaria cases also surged by 150% in the same period, while the number of deaths increased by 153%. It is worth noting that this increasing trend in malaria cases and deaths is common in 10 of the 11 malaria High Burden to High Impact countries.
Reversing the surge of malaria cases and deaths requires first understanding the root causes. Considering this, the Technical Review Panel (TRP) recommended a retrospective analysis to investigate the root causes. The investigation was completed and discussed in December 2022. Its outcomes are expected to be leveraged to inform interventions for the upcoming funding cycle.
While coverage of key interventions is good, the impact of drug-based prevention intervention does not show a steadily declining trend in the number of severe malaria cases for children under five, which increased from 147,983 in 2019 to 189,067 in 2020 but then declined to 157,693 in 2021. Due to the improved quality of data in 2020 and 2021, the retrospective analysis could not draw conclusions for the period prior to 2020.
Now that the retrospective analysis has been completed, the information is being used by the Country Coordinating Mechanism (CCM) and NMCP to inform the next funding cycle’s interventions; hence, no further management action is considered necessary at this time.
Second Finding
Limited progress has been achieved in improving HIV quality of care and data reporting; and issues with HIV interventions that the OIG identified in 2018 remain unaddressed. These include unreliable data on patients under antiretroviral therapy (ART), a high rate of loss to follow up patients, low viral load coverage and the poor prevention of mother-to-child transmission (PMTCT) cascade. Mitigation measures are planned, but implementation has been slow.
The OIG identified four issues that need addressing to improve HIV outcomes:
- Unreliable data of patients under ART cohort.
- Ineffective monitoring mechanism to track HIV patients no longer undergoing treatment.
- Low observance of ART.
- Low coverage of viral load monitoring.
Corrective actions have been planned to address these issues with a focus on the 26 high-volume ART clinics that account for 80% of patients. However, implementation has been delayed. The OIG noted that materials and equipment have yet to be delivered against the agreed deadline for the last quarter of 2021. Similarly, planned supervision as well as activities to track lost to follow up (LTFU) patients have not started. This is mainly due to delayed procurement processes at the MOH.
The PMTCT cascade remains poor, with OIG’s observations similar to those in the 2018 audit: (i) PMTCT testing coverage is low; (ii) the linkage from HIV testing to treatment remains low; and (iii) the coverage of early diagnosis of new-borns from HIV positive mothers is low. As a result of this weak performance, the MTCT rate remains high at 26%. A PMTCT improvement plan was developed and agreed with the Global Fund in 2022, but it has yet to be implemented.
While the mortality rate of co-infected TB/HIV patients reduced from 19% in 2020 to 14% in 2021, it remains insufficient compared to global targets. About 68% of TB patients who tested HIV positive were put under ART against a grant target of 98% in 2021. There is currently no system to track TB screening among patients under ART. These challenges reflect insufficient collaboration between the TB and HIV disease programs and the need to strengthen TB/HIV co-infection management to reduce mortality.
Considering the current estimates for key populations (KPs) by UNAIDS, the coverage of prevention and testing interventions (below 10%) is too low to achieve meaningful impact. In addition, prevention and testing activities for prison inmates started in the first semester of 2022, but outreach activities only covered 1% of the targeted population. Root causes for this low coverage include the funding gap for prevention activities, the lack of accurate KP size estimation across the country, the late normalization of HIV testing outside the capital city and the delayed implementation of an HIV differentiated testing approach.
Third Finding
The strengthening of the distribution capacity of the central medical store (ONPPC), including extending its truck fleet from three in 2018 to 15 in 2022, has allowed ONPPC to execute its distribution plan to supply district warehouses and national/regional referral hospitals in a timely manner. As a result, with some exceptions, key health commodities for the three diseases have been continuously available since 2021, at both the central level and the 16 health facilities visited. This is a key achievement that shows significant progress from the 2018 audit when the OIG noted recurring stock-outs of health products across the three diseases.
Despite the notable progress in drug availability, some key components of the supply chain still need improvement. First, the limited flow of information and coordination in the supply chain for HIV commodities has led to expiries and shortages.
Second, there has been limited consideration of the sustainability of warehouse investments and persistently inadequate storage conditions. While the OIG noted some improvement in the storage conditions, two issues still require attention: (1) high temperatures due to non-operational cooling systems; and (2) sub-optimal inventory management with data often obsolete due to issues around the continuous availability of internet connectivity.
As at the end of September 2022, the Global Fund had invested €1.08 million to rent and renovate private warehouses because the ONPCC’s warehouses were not operational despite a renovation attempt in the previous funding cycle. While the OIG does not question the current storage investment approach as a short-term solution, this approach does not support the strengthening of the existing weak health system in the long term. Discussion is ongoing between the Global Fund Secretariat and in-country stakeholders, but a decision has yet to be made by the Government on its strategy to move from the temporary storage solution to a more sustainable option, such as the acquisition of a government-owned warehouse. Furthermore, the Global Fund is putting in place a new contracting model to allow ONPCC, which is responsible for managing the rented warehouses, to bill incurred costs,
The logistics management information system (LMIS) remains dysfunctional, which hinders the visibility of stock levels and consumption at the peripheral levels. Despite training and the distribution of LMIS tools, data collection from health facilities remains ineffective due to multiple factors including: (a) the lack of a centrally accountable LMIS team in the Directorate of Pharmacy and Traditional Medicine to coordinate and monitor LMIS implementation; (b) the failure to use the web-based platform module for collecting logistics information; and (c) limited staffing.
Fourth Finding
The internal control system and the Global Fund’s assurance mechanisms for PRs are effective in preventing and detecting transaction and procurement irregularities. However, the low financial absorption of government grants has slowed down the implementation of grant activities.
Catholic Relief Services, the civil society PR, recorded financial absorption of 80% for malaria/C19RM from January 2021 to June 2022, whereas the government PR absorbed just 37% of allocated funds (HIV and RSSH interventions) during the same period. For the TB grant which started in January 2022, financial absorption was 24% in the first six months of implementation. The absorption of COVID-19 Resource Mechanism (C19RM) funds, including the HIV grant, was much lower at 5%. This low absorption suggests that grant activities experienced delays or were not implemented at all. The OIG saw evidence of this during the audit: (a) delayed implementation of the 26 HIV high volume sites project; (b) activities meant to strengthen the laboratory network were not implemented on a timely basis: (c) delayed implementation of HIV differentiated testing; and (d) the rehabilitation of three regional warehouses had not started, which would have improved drug storage conditions.
Causes for these delays include:
- The insufficient capacity of the MOH’s grant management unit (UGS) to plan, monitor and coordinate the implementation of its annual workplan has contributed to the low absorption. The workplan is unspecific about the target timelines and does not contain key information to allow proper monitoring. Coordination with implementers is also challenging in the absence of defined accountability and the lack of a framework to identify and address bottlenecks on a timely basis. Significant delays were noted in the procurement of non-health products and services: 96% and 63% of planned procurements respectively in 2022 and 2021 were either not or only partially executed with a value of €5.6 million. The OIG also noted that procurement processes took up to 10 months for completion in some instances.
- COVID-19 travel restrictions prevented the Country Team from better assessing implementation bottlenecks and identifying mitigation measures in a timely manner. For example, it took almost 15 months for the Secretariat to propose a solution to address the slow disbursement of funds to sub-implementers, one of the main contributors to low absorption.
- The validation of expenditures is time-consuming and impacts fund absorption. The OIG found that 60% of expenditure or request for payments submitted every quarter by the UGS could not be approved by the Fiscal Agent on first submission. Most were due to incomplete or inconsistent supporting documents, which can take up to two months for implementers to address and to get the payment validated. No remediation plan had been proposed by any of the parties involved at the time of the audit.
Audit Ratings
The audit’s overall objective was to provide reasonable assurance on the adequacy, effectiveness, and efficiency of Global Fund Grants to the Republic of Niger. The assessment of the three specific audit objectives were:
Table C: Audit Objectives and Ratings
|
Objective |
Rating |
|
The existing implementation arrangement at the Ministry of Health, as well as the design and implementation of key program interventions particularly: the quality of services and the health information management system. |
Needs significant improvement |
|
The design and implementation of mitigation measures to ensure continuous availability of quality-assured health commodities, efficiency, and accountability across the supply chain. |
Partially effective |
|
Implementers’ financial management system, as well as an assurance mechanism to mitigate financial and fiduciary risks and to allow efficient implementation of grant activities. |
Partially effective |
Agreed Management Actions
The agreed management actions (AMAs) for findings 2, 3 and 4 are as follows:
2. The Secretariat in conjunction with the MOH and partners will ensure that by 30 September 2024:
(a) An ART register that allows for the monitoring the ART cohort, including adherence to treatment, tracking of LTFU and retention in care, specific treatment regimen, etc., is validated and deployed in the high-volume ART sites representing over 80% of the cohort; and
(b) High burden PMTCT sites supported through the strategic initiative TA are strengthened to provide quality PMTCT services through the implementation of a package of interventions including refresher trainings for health providers and PMTCT/HIV focal points on basic integration of PMTCT services in prenatal consultation and mentoring of health providers by a pool of PMTCT mentors.
3. The Secretariat will work with the MOH, partners and implementers so that by 30 June 2024:
(a) a Logistics Management Unit (LMU) has been set up within the MOH’s Directorate of Pharmacy (currently being moved into a newly established Pharma Regulatory Agency) to strengthen governance and supervision of the LMIS monitoring HIV program commodities management; and
(b) the identified gaps in storage conditions and inventory management at central level have been addressed.
4. The Secretariat will work with implementers to define, by 30 April 2024, key performance indictors (KPIs) at the UGS level to monitor the efficiency of financial and non-health procurement processes.
Commentary
This audit report is about the Global Fund grants. Even so, it would have been useful to mention the total disease program budgets and the contributions from the government and any other sources. Has the government met its financial commitments?
In the First Finding, concerning malaria, the report refers to the “surge in cases and deaths since 2017”. That appears to be something of an over-statement. First, there have been greater surges in cases in the past (in 2012, 2014 and 2016) – see Table D below. Second, as the table shows, in 2021 the number of deaths as a percentage of the population was below that of 2017. Given the disruption to the health system caused by the COVID-19 pandemic, the malaria indicators are probably better that might have been expected. We look forward with interest to the findings of the retrospective analysis.
Table D: Malaria Cases in Niger 2020-2021
|
Year |
Suspected Cases |
Presumed and Confirmed |
Estimated Deaths |
||
|
Cases |
% of Population |
Number |
% of Population |
||
|
2010 |
11,231,308 |
4,231,896 |
25.42 |
26,471 |
0.159 |
|
2011 |
5,315,184 |
4,401,099 |
25.46 |
28,225 |
0.163 |
|
2012 |
7,818,305 |
6,398,943 |
35.64 |
28,977 |
0.161 |
|
2013 |
5,584,223 |
4,333,905 |
23.23 |
28,864 |
0.155 |
|
2014 |
7,100,212 |
5,247,235 |
27.07 |
27,969 |
0.144 |
|
2015 |
4,671,411 |
3,937,742 |
19.56 |
26,184 |
0.130 |
|
2016 |
7,347,200 |
5,166,336 |
24.69 |
26,110 |
0.125 |
|
2017 |
4,013,178 |
2,761,268 |
12.70 |
23,815 |
0.110 |
|
2018 |
4,810,919 |
3,358,058 |
14.87 |
22,047 |
0.098 |
|
2019 |
5,582,958 |
3,771,451 |
16.09 |
22,568 |
0.096 |
|
2020 |
6,343,569 |
4,377,938 |
17.99 |
24,068 |
0.099 |
|
2021 |
6,472,227 |
4,659,909 |
18.45 |
24,997 |
0.099 |
Source: World Malaria Report 2022, WHO.
The Second and Third Findings certainly make sense. However, perhaps some allowances – or at least mention – should have been made for the effects, albeit unquantifiable, of the COVID-19 pandemic. According to OIG:
“As for the programmatic results in Finding 2, the OIG did not consider the pandemic effect to be relevant for the issue. The observations pertain to trends that date to before the beginning of the pandemic or are unrelated, e.g. the retrospective analysis could have been carried out despite the pandemic, and observations from 2018 should have been addressed prior to 2020. Regarding Finding 3 the OIG highlights weaknesses that have no direct relation with the pandemic, i.e. the activation of the cooling system which is installed since months and was still awaiting to be turned on, and the Strategic decision by the Global Fund to favour external solutions.”
The Third AMA mentions the setting up of the LMU which is part of a directorate that is being set up separately as a regulatory agency. That sounds like a recipe for delay; and, given that Niger is classified as a COE, there is the risk that this regulatory body will be ineffective. Interestingly, the report does not refer to any aspects of the COE and ASP that have affected disease program performance or factored into the OIG’s ratings. However, according to OIG:
“The Ministry of Public Health, Population and Social Affairs has successfully transformed, through an institutional reform, the Pharmacy Directorate into the Nigerian Agency for the Regulation of the Pharmaceutical Sector (ANRP) in accordance with regional/sub-regional (WAEMU, ECOWAS) and African Union requirements. The Agency is placed under the technical supervision of the Minister of Public Health and under the financial supervision of the Minister of Finance and managed by a Board. The staff of the Directorate of Pharmacy has been entirely transferred to the Agency. The staffing of the LMU is underway. The Niger’s classification as COE by the GF does not add any additional risk to the effectiveness or ineffectiveness of the processes.”
AMA 4 is confusing. It refers to the PMU in the Ministry of Public Health, Population and Social Affairs (understandably shortened to ‘Ministry of Health’); but there has been no previous mention of a PMU. This is because “Grant management unit” is the literal translation from the French terminology and the acronym (UGS) used to refer to the PMU (English language terminology). More importantly, this AMA is about setting KPIs “to monitor the efficiency of financial and non-health procurement processes” which, given the many years of Global Fund support, should have been in place long ago. Yet, according to the AMA timetable, it is going to take another year to define those KPIs! Why so long? More importantly, the AMA is only to define KPIs whereas the need is action to improve the grant absorption rate. OIG’s explanation for this AMA and its timing is:
“The KPIs will be defined based on the work that has been ongoing in GC6, thanks to TA in place with support from Expertise France. to strengthen the program management capacities of the PMU, particularly planning, management and coordination of implementing entities and financial management. The timeline given by the OIG is for setting up a formal KPI monitoring system and then allowing for sufficient time to make sure it is working and supporting the overall goal of improving grant performance.”
Finally, in the executive summary opinion it states that the Country Team did not leverage enough the financial flexibilities to maximize the use of Global Fund grants. However, the only reference to this in the final paragraph of the report notes which ends by stating that “Given the known insecurities and challenging conditions in some areas, further leveraging of these flexibilities could improve timely implementation of activities in certain areas”. However, this does not explain what flexibilities could or should have been leveraged and what additional amounts they could have realised.
